Nassim Matin, Kasra Sarhadi, C Patrick Crooks, Abhijit V Lele, Vasisht Srinivasan, Nicholas J Johnson, Chiara Robba, James A Town, Sarah Wahlster
{"title":"脑肺串扰:严重急性脑损伤和急性呼吸窘迫综合征并发症的处理。","authors":"Nassim Matin, Kasra Sarhadi, C Patrick Crooks, Abhijit V Lele, Vasisht Srinivasan, Nicholas J Johnson, Chiara Robba, James A Town, Sarah Wahlster","doi":"10.1007/s11940-022-00726-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose of review: </strong>To summarize pathophysiology, key conflicts, and therapeutic approaches in managing concomitant severe acute brain injury (SABI) and acute respiratory distress syndrome (ARDS).</p><p><strong>Recent findings: </strong>ARDS is common in SABI and independently associated with worse outcomes in all SABI subtypes. Most landmark ARDS trials excluded patients with SABI, and evidence to guide decisions is limited in this population. Potential areas of conflict in the management of patients with both SABI and ARDS are (1) risk of intracranial pressure (ICP) elevation with high levels of positive end-expiratory pressure (PEEP), permissive hypercapnia due to lung protective ventilation (LPV), or prone ventilation; (2) balancing a conservative fluid management strategy with ensuring adequate cerebral perfusion, particularly in patients with symptomatic vasospasm or impaired cerebrovascular blood flow; and (3) uncertainty about the benefit and harm of corticosteroids in this population, with a mortality benefit in ARDS, increased mortality shown in TBI, and conflicting data in other SABI subtypes. Also, the widely adapted partial pressure of oxygen (P<sub>a</sub>O<sub>2</sub>) target of > 55 mmHg for ARDS may exacerbate secondary brain injury, and recent guidelines recommend higher goals of 80-120 mmHg in SABI. Distinct pathophysiology and trajectories among different SABI subtypes need to be considered.</p><p><strong>Summary: </strong>The management of SABI with ARDS is highly complex, and conventional ARDS management strategies may result in increased ICP and decreased cerebral perfusion. A crucial aspect of concurrent management is to recognize the risk of secondary brain injury in the individual patient, monitor with vigilance, and adjust management during critical time windows. The care of these patients requires meticulous attention to oxygenation and ventilation, hemodynamics, temperature management, and the neurological exam. LPV and prone ventilation should be utilized, and supplemented with invasive ICP monitoring if there is concern for cerebral edema and increased ICP. PEEP titration should be deliberate, involving measures of hemodynamic, pulmonary, and brain physiology. Serial volume status assessments should be performed in SABI and ARDS, and fluid management should be individualized based on measures of brain perfusion, the neurological exam, and cardiopulmonary status. More research is needed to define risks and benefits in corticosteroids in this population.</p>","PeriodicalId":10975,"journal":{"name":"Current Treatment Options in Neurology","volume":"24 9","pages":"383-408"},"PeriodicalIF":1.8000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9363869/pdf/","citationCount":"0","resultStr":"{\"title\":\"Brain-Lung Crosstalk: Management of Concomitant Severe Acute Brain Injury and Acute Respiratory Distress Syndrome.\",\"authors\":\"Nassim Matin, Kasra Sarhadi, C Patrick Crooks, Abhijit V Lele, Vasisht Srinivasan, Nicholas J Johnson, Chiara Robba, James A Town, Sarah Wahlster\",\"doi\":\"10.1007/s11940-022-00726-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose of review: </strong>To summarize pathophysiology, key conflicts, and therapeutic approaches in managing concomitant severe acute brain injury (SABI) and acute respiratory distress syndrome (ARDS).</p><p><strong>Recent findings: </strong>ARDS is common in SABI and independently associated with worse outcomes in all SABI subtypes. Most landmark ARDS trials excluded patients with SABI, and evidence to guide decisions is limited in this population. Potential areas of conflict in the management of patients with both SABI and ARDS are (1) risk of intracranial pressure (ICP) elevation with high levels of positive end-expiratory pressure (PEEP), permissive hypercapnia due to lung protective ventilation (LPV), or prone ventilation; (2) balancing a conservative fluid management strategy with ensuring adequate cerebral perfusion, particularly in patients with symptomatic vasospasm or impaired cerebrovascular blood flow; and (3) uncertainty about the benefit and harm of corticosteroids in this population, with a mortality benefit in ARDS, increased mortality shown in TBI, and conflicting data in other SABI subtypes. Also, the widely adapted partial pressure of oxygen (P<sub>a</sub>O<sub>2</sub>) target of > 55 mmHg for ARDS may exacerbate secondary brain injury, and recent guidelines recommend higher goals of 80-120 mmHg in SABI. Distinct pathophysiology and trajectories among different SABI subtypes need to be considered.</p><p><strong>Summary: </strong>The management of SABI with ARDS is highly complex, and conventional ARDS management strategies may result in increased ICP and decreased cerebral perfusion. A crucial aspect of concurrent management is to recognize the risk of secondary brain injury in the individual patient, monitor with vigilance, and adjust management during critical time windows. The care of these patients requires meticulous attention to oxygenation and ventilation, hemodynamics, temperature management, and the neurological exam. LPV and prone ventilation should be utilized, and supplemented with invasive ICP monitoring if there is concern for cerebral edema and increased ICP. PEEP titration should be deliberate, involving measures of hemodynamic, pulmonary, and brain physiology. Serial volume status assessments should be performed in SABI and ARDS, and fluid management should be individualized based on measures of brain perfusion, the neurological exam, and cardiopulmonary status. More research is needed to define risks and benefits in corticosteroids in this population.</p>\",\"PeriodicalId\":10975,\"journal\":{\"name\":\"Current Treatment Options in Neurology\",\"volume\":\"24 9\",\"pages\":\"383-408\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9363869/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Current Treatment Options in Neurology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s11940-022-00726-3\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/8/10 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Treatment Options in Neurology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11940-022-00726-3","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/8/10 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
Brain-Lung Crosstalk: Management of Concomitant Severe Acute Brain Injury and Acute Respiratory Distress Syndrome.
Purpose of review: To summarize pathophysiology, key conflicts, and therapeutic approaches in managing concomitant severe acute brain injury (SABI) and acute respiratory distress syndrome (ARDS).
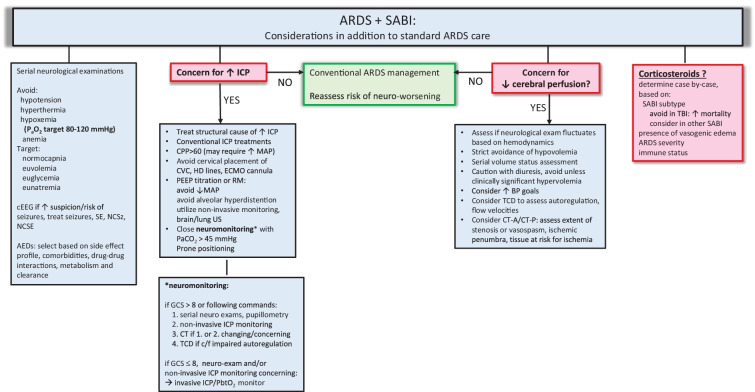
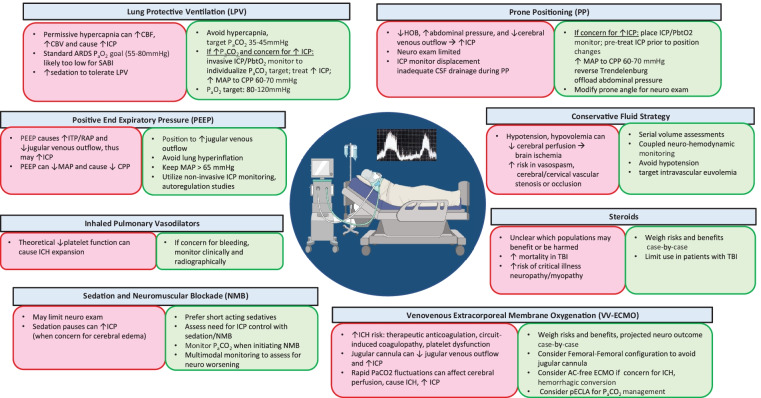
Recent findings: ARDS is common in SABI and independently associated with worse outcomes in all SABI subtypes. Most landmark ARDS trials excluded patients with SABI, and evidence to guide decisions is limited in this population. Potential areas of conflict in the management of patients with both SABI and ARDS are (1) risk of intracranial pressure (ICP) elevation with high levels of positive end-expiratory pressure (PEEP), permissive hypercapnia due to lung protective ventilation (LPV), or prone ventilation; (2) balancing a conservative fluid management strategy with ensuring adequate cerebral perfusion, particularly in patients with symptomatic vasospasm or impaired cerebrovascular blood flow; and (3) uncertainty about the benefit and harm of corticosteroids in this population, with a mortality benefit in ARDS, increased mortality shown in TBI, and conflicting data in other SABI subtypes. Also, the widely adapted partial pressure of oxygen (PaO2) target of > 55 mmHg for ARDS may exacerbate secondary brain injury, and recent guidelines recommend higher goals of 80-120 mmHg in SABI. Distinct pathophysiology and trajectories among different SABI subtypes need to be considered.
Summary: The management of SABI with ARDS is highly complex, and conventional ARDS management strategies may result in increased ICP and decreased cerebral perfusion. A crucial aspect of concurrent management is to recognize the risk of secondary brain injury in the individual patient, monitor with vigilance, and adjust management during critical time windows. The care of these patients requires meticulous attention to oxygenation and ventilation, hemodynamics, temperature management, and the neurological exam. LPV and prone ventilation should be utilized, and supplemented with invasive ICP monitoring if there is concern for cerebral edema and increased ICP. PEEP titration should be deliberate, involving measures of hemodynamic, pulmonary, and brain physiology. Serial volume status assessments should be performed in SABI and ARDS, and fluid management should be individualized based on measures of brain perfusion, the neurological exam, and cardiopulmonary status. More research is needed to define risks and benefits in corticosteroids in this population.
期刊介绍:
This journal aims to review the most important, recently published treatment option advances in the field of neurology. By presenting clear, insightful, balanced contributions by international experts, the journal intends to facilitate worldwide approaches to the treatment of neurologic conditions.
We accomplish this aim by appointing international authorities to serve as Section Editors in key subject areas, such as epilepsy, headache, neurologic ophthalmology and otology, neuromuscular disorders, psychiatric manifestations of neurologic disease, and sleep disorders. Section Editors select topics for which leading experts contribute comprehensive review articles that emphasize new developments and recently published papers of major importance, highlighted by annotated reference lists. We also provide commentaries from well-known neurologists, and an international Editorial Board reviews the annual table of contents, suggests articles of special interest to their country/region, and ensures that topics are current and include emerging research.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


