Fernando Albuquerque de Almeida, Isaac Corro Ramos, Maiwenn Al, Maureen Rutten-van Mölken
{"title":"荷兰心力衰竭管理中的家庭远程监控和诊断算法:成本效益分析。","authors":"Fernando Albuquerque de Almeida, Isaac Corro Ramos, Maiwenn Al, Maureen Rutten-van Mölken","doi":"10.2196/31302","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Heart failure is a major health concern associated with significant morbidity, mortality, and reduced quality of life in patients. Home telemonitoring (HTM) facilitates frequent or continuous assessment of disease signs and symptoms, and it has shown to improve compliance by involving patients in their own care and prevent emergency admissions by facilitating early detection of clinically significant changes. Diagnostic algorithms (DAs) are predictive mathematical relationships that make use of a wide range of collected data for calculating the likelihood of a particular event and use this output for prioritizing patients with regard to their treatment.</p><p><strong>Objective: </strong>This study aims to assess the cost-effectiveness of HTM and a DA in the management of heart failure in the Netherlands. Three interventions were analyzed: usual care, HTM, and HTM plus a DA.</p><p><strong>Methods: </strong>A previously published discrete event simulation model was used. The base-case analysis was performed according to the Dutch guidelines for economic evaluation. Sensitivity, scenario, and value of information analyses were performed. Particular attention was given to the cost-effectiveness of the DA at various levels of diagnostic accuracy of event prediction and to different patient subgroups.</p><p><strong>Results: </strong>HTM plus the DA extendedly dominates HTM alone, and it has a deterministic incremental cost-effectiveness ratio compared with usual care of €27,712 (currency conversion rate in purchasing power parity at the time of study: €1=US $1.29; further conversions are not applicable in cost-effectiveness terms) per quality-adjusted life year. The model showed robustness in the sensitivity and scenario analyses. HTM plus the DA had a 96.0% probability of being cost-effective at the appropriate €80,000 per quality-adjusted life year threshold. An optimal point for the threshold value for the alarm of the DA in terms of its cost-effectiveness was estimated. New York Heart Association class IV patients were the subgroup with the worst cost-effectiveness results versus usual care, while HTM plus the DA was found to be the most cost-effective for patients aged <65 years and for patients in New York Heart Association class I.</p><p><strong>Conclusions: </strong>Although the increased costs of adopting HTM plus the DA in the management of heart failure may seemingly be an additional strain on scarce health care resources, the results of this study demonstrate that, by increasing patient life expectancy by 1.28 years and reducing their hospitalization rate by 23% when compared with usual care, the use of this technology may be seen as an investment, as HTM plus the DA in its current form extendedly dominates HTM alone and is cost-effective compared with usual care at normally accepted thresholds in the Netherlands.</p>","PeriodicalId":14706,"journal":{"name":"JMIR Cardio","volume":" ","pages":"e31302"},"PeriodicalIF":0.0000,"publicationDate":"2022-08-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9389378/pdf/","citationCount":"0","resultStr":"{\"title\":\"Home Telemonitoring and a Diagnostic Algorithm in the Management of Heart Failure in the Netherlands: Cost-effectiveness Analysis.\",\"authors\":\"Fernando Albuquerque de Almeida, Isaac Corro Ramos, Maiwenn Al, Maureen Rutten-van Mölken\",\"doi\":\"10.2196/31302\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Heart failure is a major health concern associated with significant morbidity, mortality, and reduced quality of life in patients. Home telemonitoring (HTM) facilitates frequent or continuous assessment of disease signs and symptoms, and it has shown to improve compliance by involving patients in their own care and prevent emergency admissions by facilitating early detection of clinically significant changes. Diagnostic algorithms (DAs) are predictive mathematical relationships that make use of a wide range of collected data for calculating the likelihood of a particular event and use this output for prioritizing patients with regard to their treatment.</p><p><strong>Objective: </strong>This study aims to assess the cost-effectiveness of HTM and a DA in the management of heart failure in the Netherlands. Three interventions were analyzed: usual care, HTM, and HTM plus a DA.</p><p><strong>Methods: </strong>A previously published discrete event simulation model was used. The base-case analysis was performed according to the Dutch guidelines for economic evaluation. Sensitivity, scenario, and value of information analyses were performed. Particular attention was given to the cost-effectiveness of the DA at various levels of diagnostic accuracy of event prediction and to different patient subgroups.</p><p><strong>Results: </strong>HTM plus the DA extendedly dominates HTM alone, and it has a deterministic incremental cost-effectiveness ratio compared with usual care of €27,712 (currency conversion rate in purchasing power parity at the time of study: €1=US $1.29; further conversions are not applicable in cost-effectiveness terms) per quality-adjusted life year. The model showed robustness in the sensitivity and scenario analyses. HTM plus the DA had a 96.0% probability of being cost-effective at the appropriate €80,000 per quality-adjusted life year threshold. An optimal point for the threshold value for the alarm of the DA in terms of its cost-effectiveness was estimated. New York Heart Association class IV patients were the subgroup with the worst cost-effectiveness results versus usual care, while HTM plus the DA was found to be the most cost-effective for patients aged <65 years and for patients in New York Heart Association class I.</p><p><strong>Conclusions: </strong>Although the increased costs of adopting HTM plus the DA in the management of heart failure may seemingly be an additional strain on scarce health care resources, the results of this study demonstrate that, by increasing patient life expectancy by 1.28 years and reducing their hospitalization rate by 23% when compared with usual care, the use of this technology may be seen as an investment, as HTM plus the DA in its current form extendedly dominates HTM alone and is cost-effective compared with usual care at normally accepted thresholds in the Netherlands.</p>\",\"PeriodicalId\":14706,\"journal\":{\"name\":\"JMIR Cardio\",\"volume\":\" \",\"pages\":\"e31302\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-08-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9389378/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JMIR Cardio\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2196/31302\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR Cardio","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/31302","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
背景:心力衰竭是一个主要的健康问题,与严重的发病率、死亡率和患者生活质量下降有关。家庭远程监护(HTM)有助于频繁或持续地评估疾病的体征和症状,并通过让患者参与自身护理来提高依从性,以及通过及早发现临床重大变化来防止急诊入院。诊断算法(DAs)是一种预测性数学关系,它利用广泛收集的数据来计算特定事件发生的可能性,并利用这一输出结果来确定患者治疗的优先次序:本研究旨在评估 HTM 和 DA 在荷兰心力衰竭治疗中的成本效益。分析了三种干预措施:常规护理、HTM 和 HTM 加 DA:方法:使用之前发布的离散事件模拟模型。基础案例分析根据荷兰经济评估指南进行。进行了敏感性、情景和信息价值分析。特别关注了DA在不同事件预测诊断准确性水平和不同患者亚群中的成本效益:HTM加DA扩大了单用HTM的优势,与常规护理相比,它的确定性增量成本效益比为每质量调整生命年27712欧元(研究时的购买力平价货币兑换率:1欧元=1.29美元;进一步的兑换在成本效益方面不适用)。该模型在敏感性和情景分析中表现出稳健性。在每质量调整生命年 80,000 欧元的适当阈值下,HTM 加 DA 具有 96.0% 的成本效益概率。据估计,DA 在成本效益方面的报警阈值有一个最佳点。与常规护理相比,纽约心脏协会 IV 级患者是成本效益最差的亚组,而 HTM 加 DA 对结论年龄段的患者最具成本效益:虽然在心衰管理中采用 HTM 加 DA 所增加的成本似乎会对稀缺的医疗资源造成额外的压力,但本研究的结果表明,与常规护理相比,患者的预期寿命延长了 1.28 年,住院率降低了 23%,因此可以将这项技术的使用视为一种投资,因为目前形式的 HTM 加 DA 在单独使用 HTM 的情况下占优势,而且在荷兰,与常规护理相比,在通常接受的阈值下具有成本效益。
Home Telemonitoring and a Diagnostic Algorithm in the Management of Heart Failure in the Netherlands: Cost-effectiveness Analysis.
Background: Heart failure is a major health concern associated with significant morbidity, mortality, and reduced quality of life in patients. Home telemonitoring (HTM) facilitates frequent or continuous assessment of disease signs and symptoms, and it has shown to improve compliance by involving patients in their own care and prevent emergency admissions by facilitating early detection of clinically significant changes. Diagnostic algorithms (DAs) are predictive mathematical relationships that make use of a wide range of collected data for calculating the likelihood of a particular event and use this output for prioritizing patients with regard to their treatment.
Objective: This study aims to assess the cost-effectiveness of HTM and a DA in the management of heart failure in the Netherlands. Three interventions were analyzed: usual care, HTM, and HTM plus a DA.
Methods: A previously published discrete event simulation model was used. The base-case analysis was performed according to the Dutch guidelines for economic evaluation. Sensitivity, scenario, and value of information analyses were performed. Particular attention was given to the cost-effectiveness of the DA at various levels of diagnostic accuracy of event prediction and to different patient subgroups.
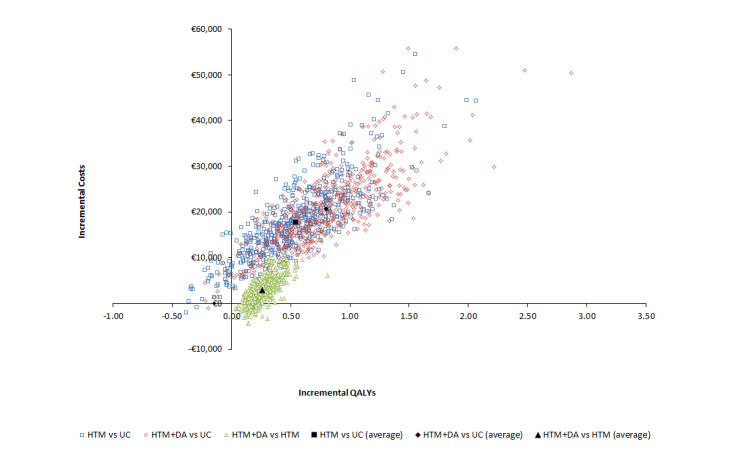
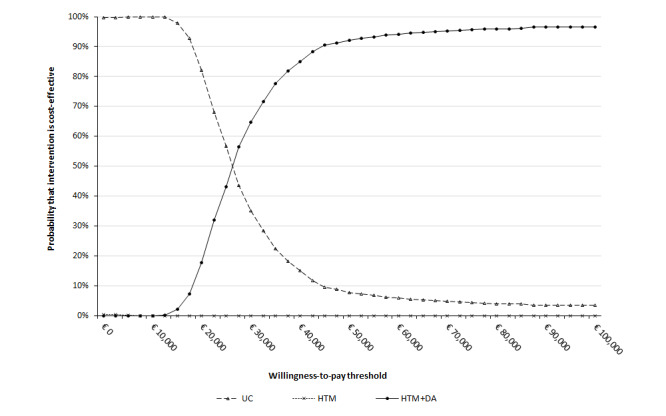
Results: HTM plus the DA extendedly dominates HTM alone, and it has a deterministic incremental cost-effectiveness ratio compared with usual care of €27,712 (currency conversion rate in purchasing power parity at the time of study: €1=US $1.29; further conversions are not applicable in cost-effectiveness terms) per quality-adjusted life year. The model showed robustness in the sensitivity and scenario analyses. HTM plus the DA had a 96.0% probability of being cost-effective at the appropriate €80,000 per quality-adjusted life year threshold. An optimal point for the threshold value for the alarm of the DA in terms of its cost-effectiveness was estimated. New York Heart Association class IV patients were the subgroup with the worst cost-effectiveness results versus usual care, while HTM plus the DA was found to be the most cost-effective for patients aged <65 years and for patients in New York Heart Association class I.
Conclusions: Although the increased costs of adopting HTM plus the DA in the management of heart failure may seemingly be an additional strain on scarce health care resources, the results of this study demonstrate that, by increasing patient life expectancy by 1.28 years and reducing their hospitalization rate by 23% when compared with usual care, the use of this technology may be seen as an investment, as HTM plus the DA in its current form extendedly dominates HTM alone and is cost-effective compared with usual care at normally accepted thresholds in the Netherlands.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


