Satish Kumar Singh, Ankit K Sahu, Akshay Kumar, L R Murmu, Sanjeev Bhoi, Praveen Aggarwal, Meera Ekka, Nayer Jamshed, Bharath Gopinath, Ghanashyam Timilsina
{"title":"中等收入国家开发的新型分流系统的前瞻性验证——AIIMS分流协议。","authors":"Satish Kumar Singh, Ankit K Sahu, Akshay Kumar, L R Murmu, Sanjeev Bhoi, Praveen Aggarwal, Meera Ekka, Nayer Jamshed, Bharath Gopinath, Ghanashyam Timilsina","doi":"10.4103/jets.jets_146_21","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Triage is a crucial process not only to identify sick patients and prioritize prompt management but also to foster efficient resource utilization. In low-and middle-income countries (LMICs) most emergency departments (ED) still have an informal triage process. Although an important element of emergency care, triage research has not been a priority in LMICs, and hence, very few triage systems have been validated. The All India Institute of Medical Sciences (AIIMS) triage protocol or ATP for adult patients was developed by expert consensus at AIIMS using the Delphi method. We attempted a prospective validation of the ATP in terms of mortality and intensive care unit (ICU)/hospital admission at 24 h.</p><p><strong>Methods: </strong>Patients presenting to the ED, who were 14 years and above were included in the study. The patients were followed up at 24 h and their outcome documented on a standardized data collection form. Mortality and ICU admission were noted at 24 h.</p><p><strong>Results: </strong>A total of 15,505 patients were recruited. After exclusion, among 13,754 patients, 6303 (45.83%) were triaged red and 7451 (54.17%) were triaged yellow. Mortality at 24 h was 10.31% (650) in red triaged patients and 0.35% (26) in yellow triaged patients. The 24-h mortality of red triaged patients was significantly higher (<i>P</i> <0.001) than that of yellow triaged patients. The presence of one or more ATP \"Red\" criteria was 96.2% (95% confidence interval [CI]: 94.42%-97.47%) sensitive and 56.8% (95% CI: 55.92%-57.63%) specific in predicting 24-h mortality. The sensitivity and specificity of ATP \"Red\" criteria for 24-h ICU admission were 98.5% (95% CI: 97.7%-99.1%) and 59.6% (95% CI: 58.8%-60.5%), respectively.</p><p><strong>Conclusion: </strong>When applied to adult nontrauma patients, ATP had a high accuracy in recognizing sick patients presenting to the ED. A time-tested and validated triage system like ATP may be a good starting point for public hospital EDs in LMICs.</p>","PeriodicalId":15692,"journal":{"name":"Journal of Emergencies, Trauma, and Shock","volume":"15 3","pages":"124-127"},"PeriodicalIF":1.2000,"publicationDate":"2022-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9639733/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prospective Validation of a Novel Triage System Developed in a Middle Income Country - AIIMS Triage Protocol.\",\"authors\":\"Satish Kumar Singh, Ankit K Sahu, Akshay Kumar, L R Murmu, Sanjeev Bhoi, Praveen Aggarwal, Meera Ekka, Nayer Jamshed, Bharath Gopinath, Ghanashyam Timilsina\",\"doi\":\"10.4103/jets.jets_146_21\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Triage is a crucial process not only to identify sick patients and prioritize prompt management but also to foster efficient resource utilization. In low-and middle-income countries (LMICs) most emergency departments (ED) still have an informal triage process. Although an important element of emergency care, triage research has not been a priority in LMICs, and hence, very few triage systems have been validated. The All India Institute of Medical Sciences (AIIMS) triage protocol or ATP for adult patients was developed by expert consensus at AIIMS using the Delphi method. We attempted a prospective validation of the ATP in terms of mortality and intensive care unit (ICU)/hospital admission at 24 h.</p><p><strong>Methods: </strong>Patients presenting to the ED, who were 14 years and above were included in the study. The patients were followed up at 24 h and their outcome documented on a standardized data collection form. Mortality and ICU admission were noted at 24 h.</p><p><strong>Results: </strong>A total of 15,505 patients were recruited. After exclusion, among 13,754 patients, 6303 (45.83%) were triaged red and 7451 (54.17%) were triaged yellow. Mortality at 24 h was 10.31% (650) in red triaged patients and 0.35% (26) in yellow triaged patients. The 24-h mortality of red triaged patients was significantly higher (<i>P</i> <0.001) than that of yellow triaged patients. The presence of one or more ATP \\\"Red\\\" criteria was 96.2% (95% confidence interval [CI]: 94.42%-97.47%) sensitive and 56.8% (95% CI: 55.92%-57.63%) specific in predicting 24-h mortality. The sensitivity and specificity of ATP \\\"Red\\\" criteria for 24-h ICU admission were 98.5% (95% CI: 97.7%-99.1%) and 59.6% (95% CI: 58.8%-60.5%), respectively.</p><p><strong>Conclusion: </strong>When applied to adult nontrauma patients, ATP had a high accuracy in recognizing sick patients presenting to the ED. A time-tested and validated triage system like ATP may be a good starting point for public hospital EDs in LMICs.</p>\",\"PeriodicalId\":15692,\"journal\":{\"name\":\"Journal of Emergencies, Trauma, and Shock\",\"volume\":\"15 3\",\"pages\":\"124-127\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2022-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9639733/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Emergencies, Trauma, and Shock\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/jets.jets_146_21\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/9/28 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Emergencies, Trauma, and Shock","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jets.jets_146_21","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/9/28 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Prospective Validation of a Novel Triage System Developed in a Middle Income Country - AIIMS Triage Protocol.
Introduction: Triage is a crucial process not only to identify sick patients and prioritize prompt management but also to foster efficient resource utilization. In low-and middle-income countries (LMICs) most emergency departments (ED) still have an informal triage process. Although an important element of emergency care, triage research has not been a priority in LMICs, and hence, very few triage systems have been validated. The All India Institute of Medical Sciences (AIIMS) triage protocol or ATP for adult patients was developed by expert consensus at AIIMS using the Delphi method. We attempted a prospective validation of the ATP in terms of mortality and intensive care unit (ICU)/hospital admission at 24 h.
Methods: Patients presenting to the ED, who were 14 years and above were included in the study. The patients were followed up at 24 h and their outcome documented on a standardized data collection form. Mortality and ICU admission were noted at 24 h.
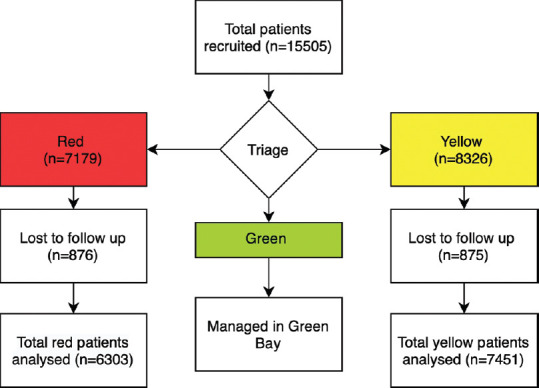
Results: A total of 15,505 patients were recruited. After exclusion, among 13,754 patients, 6303 (45.83%) were triaged red and 7451 (54.17%) were triaged yellow. Mortality at 24 h was 10.31% (650) in red triaged patients and 0.35% (26) in yellow triaged patients. The 24-h mortality of red triaged patients was significantly higher (P <0.001) than that of yellow triaged patients. The presence of one or more ATP "Red" criteria was 96.2% (95% confidence interval [CI]: 94.42%-97.47%) sensitive and 56.8% (95% CI: 55.92%-57.63%) specific in predicting 24-h mortality. The sensitivity and specificity of ATP "Red" criteria for 24-h ICU admission were 98.5% (95% CI: 97.7%-99.1%) and 59.6% (95% CI: 58.8%-60.5%), respectively.
Conclusion: When applied to adult nontrauma patients, ATP had a high accuracy in recognizing sick patients presenting to the ED. A time-tested and validated triage system like ATP may be a good starting point for public hospital EDs in LMICs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


