Antti-Pekka E Rissanen, Mirva Rottensteiner, Urho M Kujala, Jari L O Kurkela, Jan Wikgren, Jari A Laukkanen
{"title":"有心血管危险因素的成人基于心率和身体加速的心肺健康评估:验证研究。","authors":"Antti-Pekka E Rissanen, Mirva Rottensteiner, Urho M Kujala, Jari L O Kurkela, Jan Wikgren, Jari A Laukkanen","doi":"10.2196/35796","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cardiorespiratory fitness (CRF) is an independent risk factor for cardiovascular morbidity and mortality. Adding CRF to conventional risk factors (eg, smoking, hypertension, impaired glucose metabolism, and dyslipidemia) improves the prediction of an individual's risk for adverse health outcomes such as those related to cardiovascular disease. Consequently, it is recommended to determine CRF as part of individualized risk prediction. However, CRF is not determined routinely in everyday clinical practice. Wearable technologies provide a potential strategy to estimate CRF on a daily basis, and such technologies, which provide CRF estimates based on heart rate and body acceleration, have been developed. However, the validity of such technologies in estimating individual CRF in clinically relevant populations is poorly known.</p><p><strong>Objective: </strong>The objective of this study is to evaluate the validity of a wearable technology, which provides estimated CRF based on heart rate and body acceleration, in working-aged adults with cardiovascular risk factors.</p><p><strong>Methods: </strong>In total, 74 adults (age range 35-64 years; n=56, 76% were women; mean BMI 28.7, SD 4.6 kg/m<sup>2</sup>) with frequent cardiovascular risk factors (eg, n=64, 86% hypertension; n=18, 24% prediabetes; n=14, 19% type 2 diabetes; and n=51, 69% metabolic syndrome) performed a 30-minute self-paced walk on an indoor track and a cardiopulmonary exercise test on a treadmill. CRF, quantified as peak O<sub>2</sub> uptake, was both estimated (self-paced walk: a wearable single-lead electrocardiogram device worn to record continuous beat-to-beat R-R intervals and triaxial body acceleration) and measured (cardiopulmonary exercise test: ventilatory gas analysis). The accuracy of the estimated CRF was evaluated against that of the measured CRF.</p><p><strong>Results: </strong>Measured CRF averaged 30.6 (SD 6.3; range 20.1-49.6) mL/kg/min. In all participants (74/74, 100%), mean difference between estimated and measured CRF was -0.1 mL/kg/min (P=.90), mean absolute error was 3.1 mL/kg/min (95% CI 2.6-3.7), mean absolute percentage error was 10.4% (95% CI 8.5-12.5), and intraclass correlation coefficient was 0.88 (95% CI 0.80-0.92). Similar accuracy was observed in various subgroups (sexes, age, BMI categories, hypertension, prediabetes, and metabolic syndrome). However, mean absolute error was 4.2 mL/kg/min (95% CI 2.6-6.1) and mean absolute percentage error was 16.5% (95% CI 8.6-24.4) in the subgroup of patients with type 2 diabetes (14/74, 19%).</p><p><strong>Conclusions: </strong>The error of the CRF estimate, provided by the wearable technology, was likely below or at least very close to the clinically significant level of 3.5 mL/kg/min in working-aged adults with cardiovascular risk factors, but not in the relatively small subgroup of patients with type 2 diabetes. From a large-scale clinical perspective, the findings suggest that wearable technologies have the potential to estimate individual CRF with acceptable accuracy in clinically relevant populations.</p>","PeriodicalId":14706,"journal":{"name":"JMIR Cardio","volume":" ","pages":"e35796"},"PeriodicalIF":0.0000,"publicationDate":"2022-10-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9644248/pdf/","citationCount":"1","resultStr":"{\"title\":\"Cardiorespiratory Fitness Estimation Based on Heart Rate and Body Acceleration in Adults With Cardiovascular Risk Factors: Validation Study.\",\"authors\":\"Antti-Pekka E Rissanen, Mirva Rottensteiner, Urho M Kujala, Jari L O Kurkela, Jan Wikgren, Jari A Laukkanen\",\"doi\":\"10.2196/35796\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cardiorespiratory fitness (CRF) is an independent risk factor for cardiovascular morbidity and mortality. Adding CRF to conventional risk factors (eg, smoking, hypertension, impaired glucose metabolism, and dyslipidemia) improves the prediction of an individual's risk for adverse health outcomes such as those related to cardiovascular disease. Consequently, it is recommended to determine CRF as part of individualized risk prediction. However, CRF is not determined routinely in everyday clinical practice. Wearable technologies provide a potential strategy to estimate CRF on a daily basis, and such technologies, which provide CRF estimates based on heart rate and body acceleration, have been developed. However, the validity of such technologies in estimating individual CRF in clinically relevant populations is poorly known.</p><p><strong>Objective: </strong>The objective of this study is to evaluate the validity of a wearable technology, which provides estimated CRF based on heart rate and body acceleration, in working-aged adults with cardiovascular risk factors.</p><p><strong>Methods: </strong>In total, 74 adults (age range 35-64 years; n=56, 76% were women; mean BMI 28.7, SD 4.6 kg/m<sup>2</sup>) with frequent cardiovascular risk factors (eg, n=64, 86% hypertension; n=18, 24% prediabetes; n=14, 19% type 2 diabetes; and n=51, 69% metabolic syndrome) performed a 30-minute self-paced walk on an indoor track and a cardiopulmonary exercise test on a treadmill. CRF, quantified as peak O<sub>2</sub> uptake, was both estimated (self-paced walk: a wearable single-lead electrocardiogram device worn to record continuous beat-to-beat R-R intervals and triaxial body acceleration) and measured (cardiopulmonary exercise test: ventilatory gas analysis). The accuracy of the estimated CRF was evaluated against that of the measured CRF.</p><p><strong>Results: </strong>Measured CRF averaged 30.6 (SD 6.3; range 20.1-49.6) mL/kg/min. In all participants (74/74, 100%), mean difference between estimated and measured CRF was -0.1 mL/kg/min (P=.90), mean absolute error was 3.1 mL/kg/min (95% CI 2.6-3.7), mean absolute percentage error was 10.4% (95% CI 8.5-12.5), and intraclass correlation coefficient was 0.88 (95% CI 0.80-0.92). Similar accuracy was observed in various subgroups (sexes, age, BMI categories, hypertension, prediabetes, and metabolic syndrome). However, mean absolute error was 4.2 mL/kg/min (95% CI 2.6-6.1) and mean absolute percentage error was 16.5% (95% CI 8.6-24.4) in the subgroup of patients with type 2 diabetes (14/74, 19%).</p><p><strong>Conclusions: </strong>The error of the CRF estimate, provided by the wearable technology, was likely below or at least very close to the clinically significant level of 3.5 mL/kg/min in working-aged adults with cardiovascular risk factors, but not in the relatively small subgroup of patients with type 2 diabetes. From a large-scale clinical perspective, the findings suggest that wearable technologies have the potential to estimate individual CRF with acceptable accuracy in clinically relevant populations.</p>\",\"PeriodicalId\":14706,\"journal\":{\"name\":\"JMIR Cardio\",\"volume\":\" \",\"pages\":\"e35796\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-10-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9644248/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JMIR Cardio\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2196/35796\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR Cardio","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/35796","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 1
摘要
背景:心肺适能(CRF)是心血管疾病发病率和死亡率的独立危险因素。将CRF添加到常规危险因素(如吸烟、高血压、糖代谢受损和血脂异常)中,可以改善对个人不良健康结果(如与心血管疾病相关的健康结果)风险的预测。因此,建议将CRF作为个体化风险预测的一部分。然而,在日常临床实践中,CRF并不是常规的。可穿戴技术为每天估计CRF提供了一种潜在的策略,这种技术可以根据心率和身体加速度来估计CRF。然而,这些技术在临床相关人群中评估个体CRF的有效性尚不清楚。目的:本研究的目的是评估可穿戴技术的有效性,该技术可根据心率和身体加速度提供具有心血管危险因素的工作年龄成年人的CRF估计。方法:74例成人(年龄35 ~ 64岁;N =56, 76%为女性;平均BMI 28.7, SD 4.6 kg/m2),心血管危险因素较多(例如,n=64,高血压86%;N =18, 24%为前驱糖尿病;N =14, 19%为2型糖尿病;n=51, 69%代谢综合征)在室内跑道上进行30分钟的自定节奏步行,并在跑步机上进行心肺运动测试。CRF被量化为峰值氧摄取,评估(自定步走:一种可穿戴的单导联心电图设备,用于记录连续搏动R-R间隔和三轴体加速度)和测量(心肺运动试验:通气气体分析)。根据测量的CRF来评估估计CRF的准确性。结果:测量CRF平均30.6 (SD 6.3;范围:20.1-49.6)mL/kg/min。在所有参与者(74/74,100%)中,估计的CRF和测量的CRF之间的平均差异为-0.1 mL/kg/min (P= 0.90),平均绝对误差为3.1 mL/kg/min (95% CI 2.6-3.7),平均绝对百分比误差为10.4% (95% CI 8.5-12.5),类内相关系数为0.88 (95% CI 0.80-0.92)。在不同亚组(性别、年龄、BMI类别、高血压、前驱糖尿病和代谢综合征)中观察到类似的准确性。然而,2型糖尿病患者亚组的平均绝对误差为4.2 mL/kg/min (95% CI 2.6-6.1),平均绝对百分比误差为16.5% (95% CI 8.6-24.4)(14/ 74,19 %)。结论:可穿戴技术提供的CRF估计误差可能低于或至少非常接近具有心血管危险因素的工作年龄成年人的临床显著水平3.5 mL/kg/min,但在相对较小的2型糖尿病患者亚组中则不然。从大规模的临床角度来看,研究结果表明,可穿戴技术有可能在临床相关人群中以可接受的准确性估计个体CRF。
Cardiorespiratory Fitness Estimation Based on Heart Rate and Body Acceleration in Adults With Cardiovascular Risk Factors: Validation Study.
Background: Cardiorespiratory fitness (CRF) is an independent risk factor for cardiovascular morbidity and mortality. Adding CRF to conventional risk factors (eg, smoking, hypertension, impaired glucose metabolism, and dyslipidemia) improves the prediction of an individual's risk for adverse health outcomes such as those related to cardiovascular disease. Consequently, it is recommended to determine CRF as part of individualized risk prediction. However, CRF is not determined routinely in everyday clinical practice. Wearable technologies provide a potential strategy to estimate CRF on a daily basis, and such technologies, which provide CRF estimates based on heart rate and body acceleration, have been developed. However, the validity of such technologies in estimating individual CRF in clinically relevant populations is poorly known.
Objective: The objective of this study is to evaluate the validity of a wearable technology, which provides estimated CRF based on heart rate and body acceleration, in working-aged adults with cardiovascular risk factors.
Methods: In total, 74 adults (age range 35-64 years; n=56, 76% were women; mean BMI 28.7, SD 4.6 kg/m2) with frequent cardiovascular risk factors (eg, n=64, 86% hypertension; n=18, 24% prediabetes; n=14, 19% type 2 diabetes; and n=51, 69% metabolic syndrome) performed a 30-minute self-paced walk on an indoor track and a cardiopulmonary exercise test on a treadmill. CRF, quantified as peak O2 uptake, was both estimated (self-paced walk: a wearable single-lead electrocardiogram device worn to record continuous beat-to-beat R-R intervals and triaxial body acceleration) and measured (cardiopulmonary exercise test: ventilatory gas analysis). The accuracy of the estimated CRF was evaluated against that of the measured CRF.
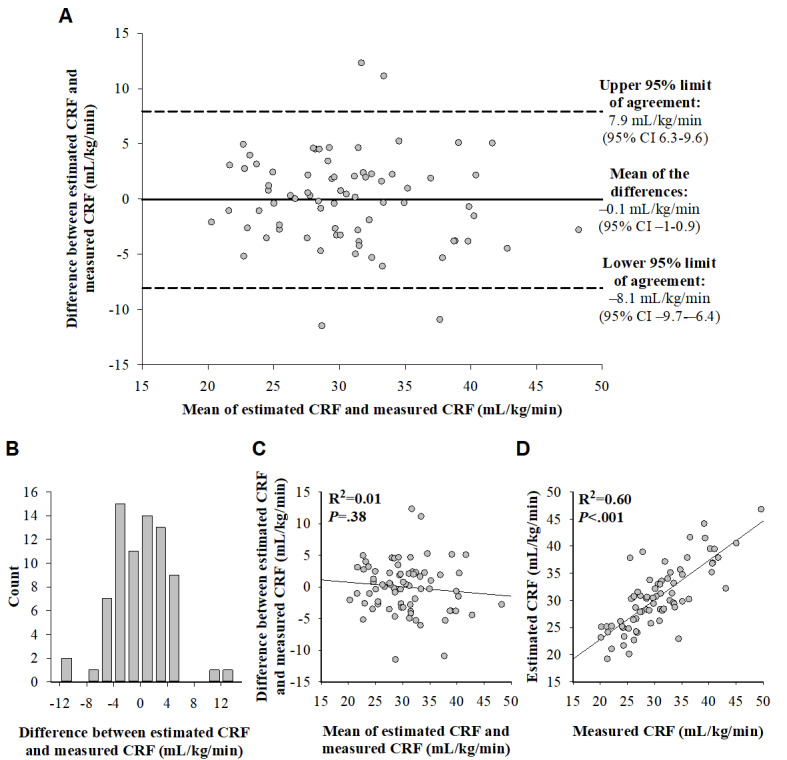
Results: Measured CRF averaged 30.6 (SD 6.3; range 20.1-49.6) mL/kg/min. In all participants (74/74, 100%), mean difference between estimated and measured CRF was -0.1 mL/kg/min (P=.90), mean absolute error was 3.1 mL/kg/min (95% CI 2.6-3.7), mean absolute percentage error was 10.4% (95% CI 8.5-12.5), and intraclass correlation coefficient was 0.88 (95% CI 0.80-0.92). Similar accuracy was observed in various subgroups (sexes, age, BMI categories, hypertension, prediabetes, and metabolic syndrome). However, mean absolute error was 4.2 mL/kg/min (95% CI 2.6-6.1) and mean absolute percentage error was 16.5% (95% CI 8.6-24.4) in the subgroup of patients with type 2 diabetes (14/74, 19%).
Conclusions: The error of the CRF estimate, provided by the wearable technology, was likely below or at least very close to the clinically significant level of 3.5 mL/kg/min in working-aged adults with cardiovascular risk factors, but not in the relatively small subgroup of patients with type 2 diabetes. From a large-scale clinical perspective, the findings suggest that wearable technologies have the potential to estimate individual CRF with acceptable accuracy in clinically relevant populations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


