{"title":"心力衰竭的性别差异。","authors":"Vera Regitz-Zagrosek","doi":"10.36628/ijhf.2020.0004","DOIUrl":null,"url":null,"abstract":"<p><p>Heart failure (HF) phenotypes differ according to sex. HF preserved ejection fraction (EF) has a greater prevalence in women and HF reduced EF (HFrEF) in men. Women with HF survive longer than men and have a lower risk of sudden death. Ischemia is the most prominent cause in men, whereas hypertension and diabetes contribute to a greater extent in women. Women with HF have a greater stiffness of the smaller left ventricle and a higher EF than men. This higher stiffness of women's hearts may be based on an increase in fibrosis at old age. In younger women estrogen reduces collagen production in female cardiac fibroblasts, but stimulates it in males. Lipid and energy metabolism is better maintained in female than in male stressed hearts. Pulse pressure is a key determinant of outcome in HF women but not in men. Takotsubo and peripartum cardiomyopathy are rare diseases affecting predominantly or exclusively women. Sudden cardiac arrest affects more men than women, but women are less adequately treated. New findings in HF therapy indicate that women with HFrEF need lower doses of beta-blockers and angiotensin-converting enzyme inhibitors than men for optimal effects. The combined neprilysin inhibitor/angiotensin II receptor blockers sacubitril-valsartan led to a significant reduction in event rate versus valsartan in women, which was not observed in men. Unfortunately, only less than 10% of recent randomized controlled trial report effects and adverse drug reactions for women and men separately. More research on sex differences in pathophysiology and therapy of HF is needed.</p>","PeriodicalId":14058,"journal":{"name":"International Journal of Heart Failure","volume":"2 3","pages":"157-181"},"PeriodicalIF":0.0000,"publicationDate":"2020-04-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0f/f3/ijhf-2-157.PMC9536682.pdf","citationCount":"30","resultStr":"{\"title\":\"Sex and Gender Differences in Heart Failure.\",\"authors\":\"Vera Regitz-Zagrosek\",\"doi\":\"10.36628/ijhf.2020.0004\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Heart failure (HF) phenotypes differ according to sex. HF preserved ejection fraction (EF) has a greater prevalence in women and HF reduced EF (HFrEF) in men. Women with HF survive longer than men and have a lower risk of sudden death. Ischemia is the most prominent cause in men, whereas hypertension and diabetes contribute to a greater extent in women. Women with HF have a greater stiffness of the smaller left ventricle and a higher EF than men. This higher stiffness of women's hearts may be based on an increase in fibrosis at old age. In younger women estrogen reduces collagen production in female cardiac fibroblasts, but stimulates it in males. Lipid and energy metabolism is better maintained in female than in male stressed hearts. Pulse pressure is a key determinant of outcome in HF women but not in men. Takotsubo and peripartum cardiomyopathy are rare diseases affecting predominantly or exclusively women. Sudden cardiac arrest affects more men than women, but women are less adequately treated. New findings in HF therapy indicate that women with HFrEF need lower doses of beta-blockers and angiotensin-converting enzyme inhibitors than men for optimal effects. The combined neprilysin inhibitor/angiotensin II receptor blockers sacubitril-valsartan led to a significant reduction in event rate versus valsartan in women, which was not observed in men. Unfortunately, only less than 10% of recent randomized controlled trial report effects and adverse drug reactions for women and men separately. More research on sex differences in pathophysiology and therapy of HF is needed.</p>\",\"PeriodicalId\":14058,\"journal\":{\"name\":\"International Journal of Heart Failure\",\"volume\":\"2 3\",\"pages\":\"157-181\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-04-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0f/f3/ijhf-2-157.PMC9536682.pdf\",\"citationCount\":\"30\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Heart Failure\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.36628/ijhf.2020.0004\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Heart Failure","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36628/ijhf.2020.0004","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
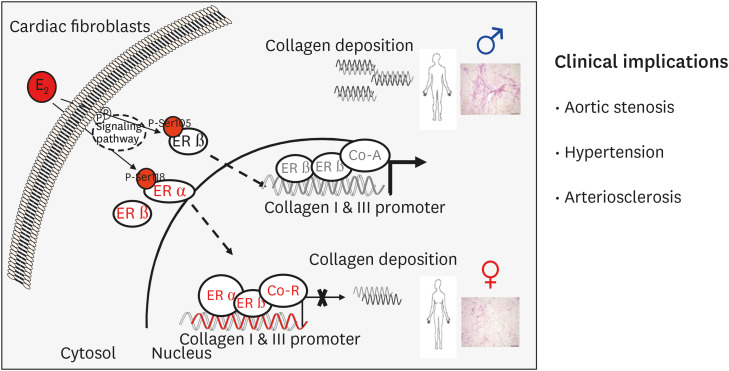
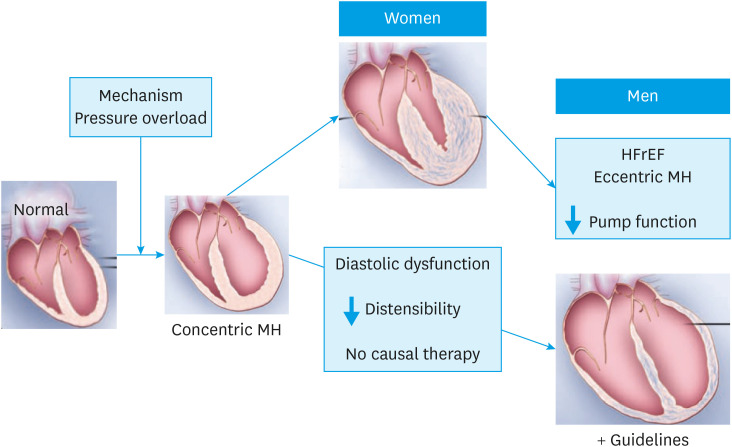
Heart failure (HF) phenotypes differ according to sex. HF preserved ejection fraction (EF) has a greater prevalence in women and HF reduced EF (HFrEF) in men. Women with HF survive longer than men and have a lower risk of sudden death. Ischemia is the most prominent cause in men, whereas hypertension and diabetes contribute to a greater extent in women. Women with HF have a greater stiffness of the smaller left ventricle and a higher EF than men. This higher stiffness of women's hearts may be based on an increase in fibrosis at old age. In younger women estrogen reduces collagen production in female cardiac fibroblasts, but stimulates it in males. Lipid and energy metabolism is better maintained in female than in male stressed hearts. Pulse pressure is a key determinant of outcome in HF women but not in men. Takotsubo and peripartum cardiomyopathy are rare diseases affecting predominantly or exclusively women. Sudden cardiac arrest affects more men than women, but women are less adequately treated. New findings in HF therapy indicate that women with HFrEF need lower doses of beta-blockers and angiotensin-converting enzyme inhibitors than men for optimal effects. The combined neprilysin inhibitor/angiotensin II receptor blockers sacubitril-valsartan led to a significant reduction in event rate versus valsartan in women, which was not observed in men. Unfortunately, only less than 10% of recent randomized controlled trial report effects and adverse drug reactions for women and men separately. More research on sex differences in pathophysiology and therapy of HF is needed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


