Nikhita Ravikanti, Hayrettin Okut, Jennifer Keomany, Elizabeth Ablah, Kent Bradley
{"title":"妇产科医生产后阿片类药物处方实践的差异。","authors":"Nikhita Ravikanti, Hayrettin Okut, Jennifer Keomany, Elizabeth Ablah, Kent Bradley","doi":"10.17161/kjm.vol15.18246","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>There have been many efforts to combat the United States opioid crisis that has been occurring for the past two decades, specifically with postpartum patients that often were prescribed opioids. Prior studies described how accounting for usage of inpatient opioids on the day prior to discharge had an impact on how much discharge opioids were prescribed on the day of discharge. These studies provided a guideline to use the inpatient opioid amount from the day before discharge to determine discharge opioid quantity and minimize how much was being prescribed. In July 2018, the American College of Obstetrics and Gynecologists (ACOG) published Committee Opinion 742, guidelines for obstetricians-gynecologists about post-partum pain management. Prescription pain medications (including opioids, if necessary) require a shared decision-making approach between the physician and patient to determine the medication type and quantity. This study aimed to determine if there were differences in prescribing practices based on the specific post-operative day that opioid prescriptions were written, and if there were differences in the prescribing practices for cesarean deliveries following the publication of ACOG Committee Opinion 742.</p><p><strong>Methods: </strong>This retrospective chart review included patients who had a live cesarean birth at one rural Midwest facility anytime between July 1, 2017 and February 28, 2021. This study excluded those with chorioamnionitis and those discharged after more than four days. Opioid amounts were converted to oral morphine milligram equivalents (MME) for comparison, and total MME was calculated for each prescription. Patients were stratified into two groups based on the day that their discharge opioid medication prescriptions were written (i.e., a day prior to discharge or the day of discharge). Patients were also stratified based on date of delivery, before or after the publication of ACOG Committee Opinion 742.</p><p><strong>Results: </strong>Of 411 cesarean patients, 93.9% (n = 386) had opioids prescribed at discharge, 86% (n = 330) of whom received a prescription written on the day of discharge. There was no difference in the quantity of MMEs, doses per day, or dosage from discharge prescriptions between those written on the day of discharge and those written on a prior day. Patients whose deliveries occurred after the publication of ACOG Committee Opinion 742 (63.9%, n = 263) received discharge prescriptions with fewer average MMEs (159.53 ± 61.64) than those whose deliveries occurred before the publication (36%, n = 148; 187.35 ± 53.42; χ<sup>2</sup> (1, N = 411) = 17.71; p < 0.001), and they were prescribed fewer doses per day.</p><p><strong>Conclusions: </strong>After cesarean sections, the specific post-operative day did not seem to impact the prescribing trends as there were no differences in MMEs, doses per day, or dosage between prescriptions that were written on the day of discharge and before the day of discharge. Patients whose deliveries occurred after the publication of ACOG Committee Opinion 742 received discharge prescriptions with fewer MMEs, fewer doses per day, and the same dosage than those whose deliveries occurred before the publication, reflecting the overall national trend of decreasing prescription opioids over these years.</p>","PeriodicalId":17991,"journal":{"name":"Kansas Journal of Medicine","volume":" ","pages":"373-379"},"PeriodicalIF":0.0000,"publicationDate":"2022-10-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/77/e3/15-373.PMC9612903.pdf","citationCount":"0","resultStr":"{\"title\":\"Variations in Postpartum Opioid Prescribing Practices among Obstetrician-Gynecologists.\",\"authors\":\"Nikhita Ravikanti, Hayrettin Okut, Jennifer Keomany, Elizabeth Ablah, Kent Bradley\",\"doi\":\"10.17161/kjm.vol15.18246\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>There have been many efforts to combat the United States opioid crisis that has been occurring for the past two decades, specifically with postpartum patients that often were prescribed opioids. Prior studies described how accounting for usage of inpatient opioids on the day prior to discharge had an impact on how much discharge opioids were prescribed on the day of discharge. These studies provided a guideline to use the inpatient opioid amount from the day before discharge to determine discharge opioid quantity and minimize how much was being prescribed. In July 2018, the American College of Obstetrics and Gynecologists (ACOG) published Committee Opinion 742, guidelines for obstetricians-gynecologists about post-partum pain management. Prescription pain medications (including opioids, if necessary) require a shared decision-making approach between the physician and patient to determine the medication type and quantity. This study aimed to determine if there were differences in prescribing practices based on the specific post-operative day that opioid prescriptions were written, and if there were differences in the prescribing practices for cesarean deliveries following the publication of ACOG Committee Opinion 742.</p><p><strong>Methods: </strong>This retrospective chart review included patients who had a live cesarean birth at one rural Midwest facility anytime between July 1, 2017 and February 28, 2021. This study excluded those with chorioamnionitis and those discharged after more than four days. Opioid amounts were converted to oral morphine milligram equivalents (MME) for comparison, and total MME was calculated for each prescription. Patients were stratified into two groups based on the day that their discharge opioid medication prescriptions were written (i.e., a day prior to discharge or the day of discharge). Patients were also stratified based on date of delivery, before or after the publication of ACOG Committee Opinion 742.</p><p><strong>Results: </strong>Of 411 cesarean patients, 93.9% (n = 386) had opioids prescribed at discharge, 86% (n = 330) of whom received a prescription written on the day of discharge. There was no difference in the quantity of MMEs, doses per day, or dosage from discharge prescriptions between those written on the day of discharge and those written on a prior day. Patients whose deliveries occurred after the publication of ACOG Committee Opinion 742 (63.9%, n = 263) received discharge prescriptions with fewer average MMEs (159.53 ± 61.64) than those whose deliveries occurred before the publication (36%, n = 148; 187.35 ± 53.42; χ<sup>2</sup> (1, N = 411) = 17.71; p < 0.001), and they were prescribed fewer doses per day.</p><p><strong>Conclusions: </strong>After cesarean sections, the specific post-operative day did not seem to impact the prescribing trends as there were no differences in MMEs, doses per day, or dosage between prescriptions that were written on the day of discharge and before the day of discharge. Patients whose deliveries occurred after the publication of ACOG Committee Opinion 742 received discharge prescriptions with fewer MMEs, fewer doses per day, and the same dosage than those whose deliveries occurred before the publication, reflecting the overall national trend of decreasing prescription opioids over these years.</p>\",\"PeriodicalId\":17991,\"journal\":{\"name\":\"Kansas Journal of Medicine\",\"volume\":\" \",\"pages\":\"373-379\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-10-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/77/e3/15-373.PMC9612903.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Kansas Journal of Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.17161/kjm.vol15.18246\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Kansas Journal of Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17161/kjm.vol15.18246","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Variations in Postpartum Opioid Prescribing Practices among Obstetrician-Gynecologists.
Introduction: There have been many efforts to combat the United States opioid crisis that has been occurring for the past two decades, specifically with postpartum patients that often were prescribed opioids. Prior studies described how accounting for usage of inpatient opioids on the day prior to discharge had an impact on how much discharge opioids were prescribed on the day of discharge. These studies provided a guideline to use the inpatient opioid amount from the day before discharge to determine discharge opioid quantity and minimize how much was being prescribed. In July 2018, the American College of Obstetrics and Gynecologists (ACOG) published Committee Opinion 742, guidelines for obstetricians-gynecologists about post-partum pain management. Prescription pain medications (including opioids, if necessary) require a shared decision-making approach between the physician and patient to determine the medication type and quantity. This study aimed to determine if there were differences in prescribing practices based on the specific post-operative day that opioid prescriptions were written, and if there were differences in the prescribing practices for cesarean deliveries following the publication of ACOG Committee Opinion 742.
Methods: This retrospective chart review included patients who had a live cesarean birth at one rural Midwest facility anytime between July 1, 2017 and February 28, 2021. This study excluded those with chorioamnionitis and those discharged after more than four days. Opioid amounts were converted to oral morphine milligram equivalents (MME) for comparison, and total MME was calculated for each prescription. Patients were stratified into two groups based on the day that their discharge opioid medication prescriptions were written (i.e., a day prior to discharge or the day of discharge). Patients were also stratified based on date of delivery, before or after the publication of ACOG Committee Opinion 742.
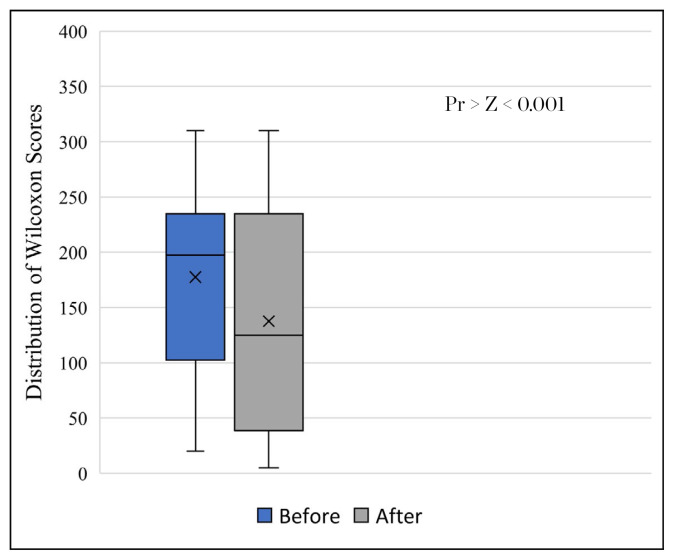
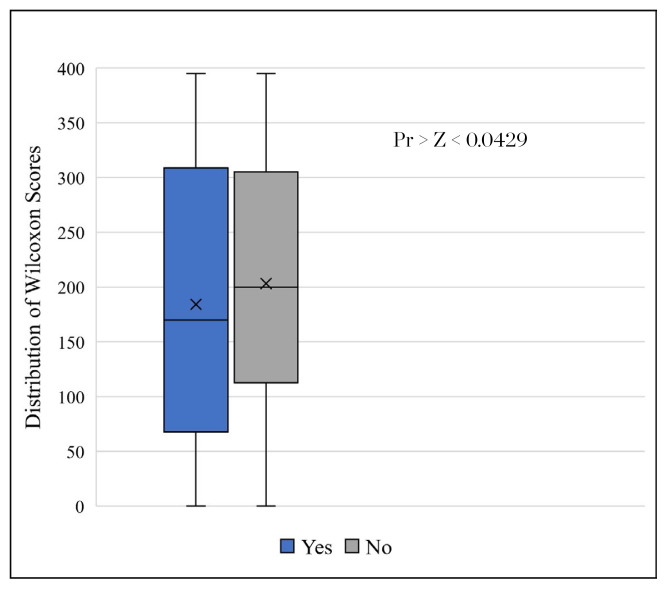
Results: Of 411 cesarean patients, 93.9% (n = 386) had opioids prescribed at discharge, 86% (n = 330) of whom received a prescription written on the day of discharge. There was no difference in the quantity of MMEs, doses per day, or dosage from discharge prescriptions between those written on the day of discharge and those written on a prior day. Patients whose deliveries occurred after the publication of ACOG Committee Opinion 742 (63.9%, n = 263) received discharge prescriptions with fewer average MMEs (159.53 ± 61.64) than those whose deliveries occurred before the publication (36%, n = 148; 187.35 ± 53.42; χ2 (1, N = 411) = 17.71; p < 0.001), and they were prescribed fewer doses per day.
Conclusions: After cesarean sections, the specific post-operative day did not seem to impact the prescribing trends as there were no differences in MMEs, doses per day, or dosage between prescriptions that were written on the day of discharge and before the day of discharge. Patients whose deliveries occurred after the publication of ACOG Committee Opinion 742 received discharge prescriptions with fewer MMEs, fewer doses per day, and the same dosage than those whose deliveries occurred before the publication, reflecting the overall national trend of decreasing prescription opioids over these years.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


