Hong Liu, Si-Chong Qian, Lu Han, Zhi-Qiang Dong, Yong-Feng Shao, Hai-Yang Li, Wei Zhang, Hong-Jia Zhang
{"title":"实验室特征区分急性A型主动脉夹层手术对低温循环骤停的耐受性。","authors":"Hong Liu, Si-Chong Qian, Lu Han, Zhi-Qiang Dong, Yong-Feng Shao, Hai-Yang Li, Wei Zhang, Hong-Jia Zhang","doi":"10.1093/icvts/ivac267","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Our goal was to investigate whether laboratory signatures on admission could be used to identify risk stratification and different tolerance to hypothermic circulatory arrest in acute type A aortic dissection surgery.</p><p><strong>Methods: </strong>Patients from 10 Chinese hospitals participating in the Additive Anti-inflammatory Action for Aortopathy & Arteriopathy (5A) study were randomly divided into derivation and validation cohorts at a ratio of 7:3 to develop and validate a simple risk score model using preoperative variables associated with in-hospital mortality using multivariable logistic regression. The performance of the model was assessed using the area under the receiver operating characteristic curve. Subgroup analyses were performed to investigate whether the laboratory signature-based risk stratification could differentiate the tolerance to hypothermic circulatory arrest.</p><p><strong>Results: </strong>There were 1443 patients and 954 patients in the derivation and validation cohorts, respectively. Multivariable analysis showed the associations of older age, larger body mass index, lower platelet-neutrophile ratio, higher lymphocyte-monocyte ratio, higher D-dimer, lower fibrinogen and lower estimated glomerular filtration rate with in-hospital death, incorporated to develop a simple risk model (5A laboratory risk score), with an area under the receiver operating characteristic of 0.736 (95% confidence interval 0.700-0.771) and 0.715 (95% CI 0.681-0.750) in the derivation and validation cohorts, respectively. Patients at low risk were more tolerant to hypothermic circulatory arrest than those at middle to high risk in terms of in-hospital mortality [odds ratio 1.814 (0.222-14.846); odds ratio 1.824 (1.137-2.926) (P = 0.996)].</p><p><strong>Conclusions: </strong>The 5A laboratory-based risk score model reflecting inflammatory, immune, coagulation and metabolic pathways provided adequate discrimination performances in in-hospital mortality prediction, which contributed to differentiating the tolerance to hypothermic circulatory arrest in acute type A aortic dissection surgery.Clinical Trials. gov number NCT04918108.</p>","PeriodicalId":13621,"journal":{"name":"Interactive cardiovascular and thoracic surgery","volume":" ","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2022-11-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/dd/f0/ivac267.PMC9645440.pdf","citationCount":"0","resultStr":"{\"title\":\"Laboratory signatures differentiate the tolerance to hypothermic circulatory arrest in acute type A aortic dissection surgery.\",\"authors\":\"Hong Liu, Si-Chong Qian, Lu Han, Zhi-Qiang Dong, Yong-Feng Shao, Hai-Yang Li, Wei Zhang, Hong-Jia Zhang\",\"doi\":\"10.1093/icvts/ivac267\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Our goal was to investigate whether laboratory signatures on admission could be used to identify risk stratification and different tolerance to hypothermic circulatory arrest in acute type A aortic dissection surgery.</p><p><strong>Methods: </strong>Patients from 10 Chinese hospitals participating in the Additive Anti-inflammatory Action for Aortopathy & Arteriopathy (5A) study were randomly divided into derivation and validation cohorts at a ratio of 7:3 to develop and validate a simple risk score model using preoperative variables associated with in-hospital mortality using multivariable logistic regression. The performance of the model was assessed using the area under the receiver operating characteristic curve. Subgroup analyses were performed to investigate whether the laboratory signature-based risk stratification could differentiate the tolerance to hypothermic circulatory arrest.</p><p><strong>Results: </strong>There were 1443 patients and 954 patients in the derivation and validation cohorts, respectively. Multivariable analysis showed the associations of older age, larger body mass index, lower platelet-neutrophile ratio, higher lymphocyte-monocyte ratio, higher D-dimer, lower fibrinogen and lower estimated glomerular filtration rate with in-hospital death, incorporated to develop a simple risk model (5A laboratory risk score), with an area under the receiver operating characteristic of 0.736 (95% confidence interval 0.700-0.771) and 0.715 (95% CI 0.681-0.750) in the derivation and validation cohorts, respectively. Patients at low risk were more tolerant to hypothermic circulatory arrest than those at middle to high risk in terms of in-hospital mortality [odds ratio 1.814 (0.222-14.846); odds ratio 1.824 (1.137-2.926) (P = 0.996)].</p><p><strong>Conclusions: </strong>The 5A laboratory-based risk score model reflecting inflammatory, immune, coagulation and metabolic pathways provided adequate discrimination performances in in-hospital mortality prediction, which contributed to differentiating the tolerance to hypothermic circulatory arrest in acute type A aortic dissection surgery.Clinical Trials. gov number NCT04918108.</p>\",\"PeriodicalId\":13621,\"journal\":{\"name\":\"Interactive cardiovascular and thoracic surgery\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2022-11-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/dd/f0/ivac267.PMC9645440.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Interactive cardiovascular and thoracic surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/icvts/ivac267\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interactive cardiovascular and thoracic surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/icvts/ivac267","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Laboratory signatures differentiate the tolerance to hypothermic circulatory arrest in acute type A aortic dissection surgery.
Objectives: Our goal was to investigate whether laboratory signatures on admission could be used to identify risk stratification and different tolerance to hypothermic circulatory arrest in acute type A aortic dissection surgery.
Methods: Patients from 10 Chinese hospitals participating in the Additive Anti-inflammatory Action for Aortopathy & Arteriopathy (5A) study were randomly divided into derivation and validation cohorts at a ratio of 7:3 to develop and validate a simple risk score model using preoperative variables associated with in-hospital mortality using multivariable logistic regression. The performance of the model was assessed using the area under the receiver operating characteristic curve. Subgroup analyses were performed to investigate whether the laboratory signature-based risk stratification could differentiate the tolerance to hypothermic circulatory arrest.
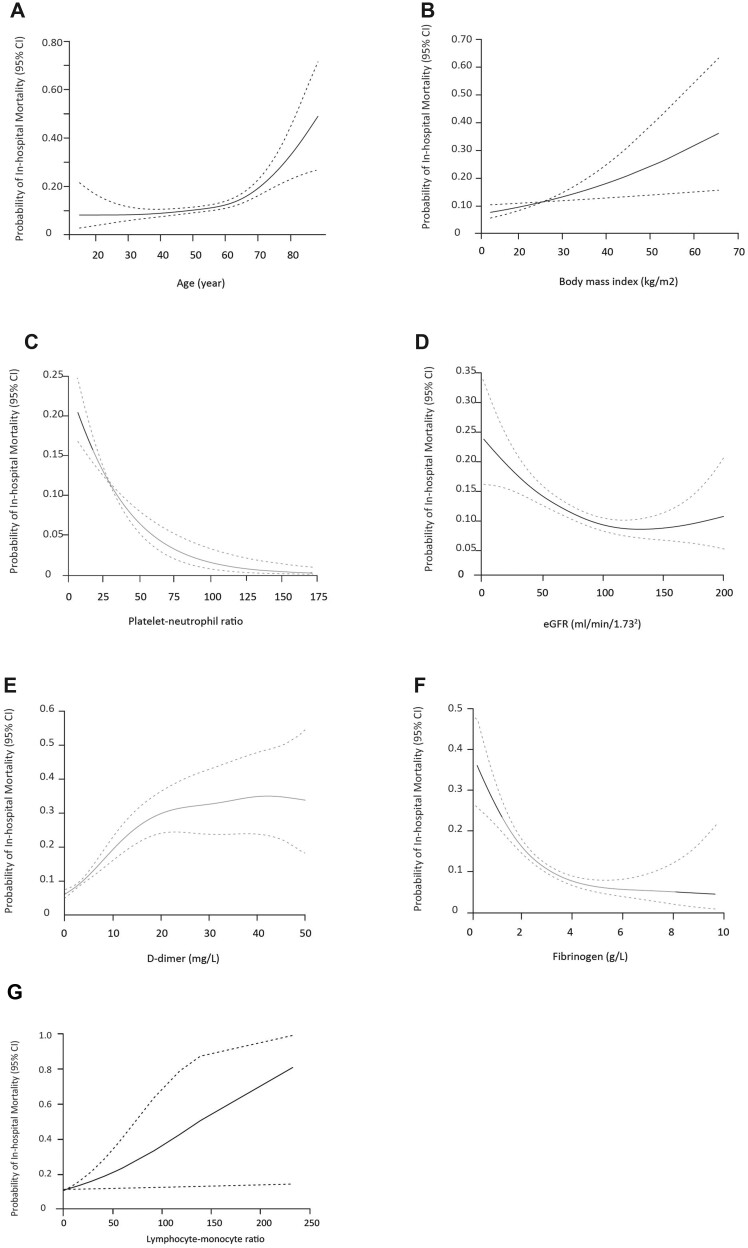
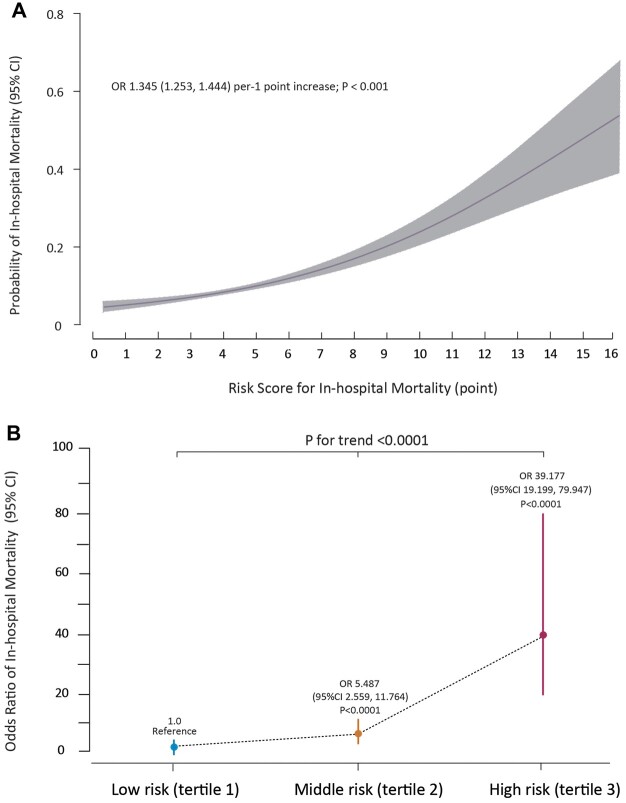
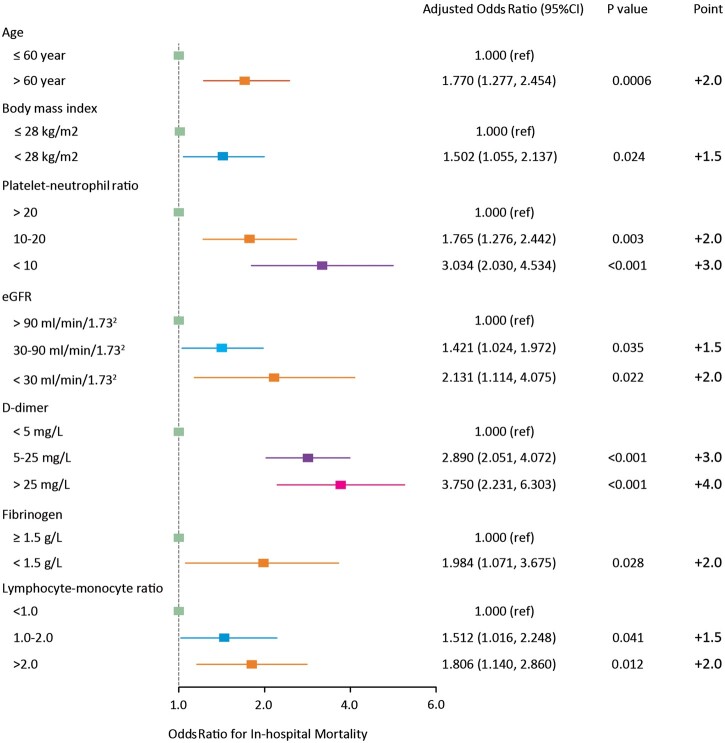
Results: There were 1443 patients and 954 patients in the derivation and validation cohorts, respectively. Multivariable analysis showed the associations of older age, larger body mass index, lower platelet-neutrophile ratio, higher lymphocyte-monocyte ratio, higher D-dimer, lower fibrinogen and lower estimated glomerular filtration rate with in-hospital death, incorporated to develop a simple risk model (5A laboratory risk score), with an area under the receiver operating characteristic of 0.736 (95% confidence interval 0.700-0.771) and 0.715 (95% CI 0.681-0.750) in the derivation and validation cohorts, respectively. Patients at low risk were more tolerant to hypothermic circulatory arrest than those at middle to high risk in terms of in-hospital mortality [odds ratio 1.814 (0.222-14.846); odds ratio 1.824 (1.137-2.926) (P = 0.996)].
Conclusions: The 5A laboratory-based risk score model reflecting inflammatory, immune, coagulation and metabolic pathways provided adequate discrimination performances in in-hospital mortality prediction, which contributed to differentiating the tolerance to hypothermic circulatory arrest in acute type A aortic dissection surgery.Clinical Trials. gov number NCT04918108.
期刊介绍:
Interactive CardioVascular and Thoracic Surgery (ICVTS) publishes scientific contributions in the field of cardiovascular and thoracic surgery, covering all aspects of surgery of the heart, vessels and the chest. The journal publishes a range of article types including: Best Evidence Topics; Brief Communications; Case Reports; Original Articles; State-of-the-Art; Work in Progress Report.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


