{"title":"腹主动脉瘤患者的血管内与开放式修复:日本基于索赔的数据分析","authors":"Yuki Kimura, Hiroshi Ohtsu, Naohiro Yonemoto, Nobuyoshi Azuma, Kazuhiro Sase","doi":"10.1136/bmjsit-2022-000131","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Endovascular aortic repair (EVAR) evolved through competition with open aortic repair (OAR) as a safe and effective treatment option for appropriately selected patients with abdominal aortic aneurysm (AAA). Although endoleaks are the most common reason for post-EVAR reintervention, compliance with lifelong regular follow-up imaging remains a challenge.</p><p><strong>Design: </strong>Retrospective data analysis.</p><p><strong>Setting: </strong>The Japan Medical Data Center (JMDC), a claims database with anonymous data linkage across hospitals, consists of corporate employees and their families of ≤75 years of age.</p><p><strong>Participants: </strong>The analysis included participants in the JMDC who underwent EVAR or OAR for intact (iAAA) or ruptured (rAAA) AAA. Patients with less than 6 months of records before the aortic repair were excluded.</p><p><strong>Main outcome measures: </strong>Overall survival and reintervention rates.</p><p><strong>Results: </strong>We identified 986 cases (837 iAAA and 149 rAAA) from JMDC with first aortic repairs between January 2015 and December 2020. The number of patients, median age (years (IQR)), follow-up (months) and post-procedure CT scan (times per year) were as follows: iAAA (OAR: n=593, 62.0 (57.0-67.0), 26.0, 1.6, EVAR: n=244, 65.0 (31.0-69.0), 17.0, 2.2), rAAA (OAR: n=110, 59.0 (53.0-59.0), 16.0, 2.1, EVAR: n=39, 62.0 (31.0-67.0), 18.0, 2.4). Reintervention rate was significantly higher among EVAR than OAR in rAAA (15.4% vs 8.2%, p=0.04). In iAAA, there were no group difference after 5 years (7.8% vs 11.0%, p=0.28), even though EVAR had initial advantage. There were no differences in mortality rate between EVAR and OAR for either rAAA or iAAA.</p><p><strong>Conclusions: </strong>Claims-based analysis in Japan showed no statistically significant difference in 5-year survival rates of the OAR and EVAR groups. However, the reintervention rate of EVAR in rAAA was significantly higher, suggesting the need for regular post-EVAR follow-up with imaging. Therefore, international collaborations for long-term outcome studies with real-world data are warranted.</p>","PeriodicalId":33349,"journal":{"name":"BMJ Surgery Interventions Health Technologies","volume":" ","pages":"e000131"},"PeriodicalIF":1.6000,"publicationDate":"2022-07-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/31/5d/bmjsit-2022-000131.PMC9345055.pdf","citationCount":"0","resultStr":"{\"title\":\"Endovascular versus open repair in patients with abdominal aortic aneurysm: a claims-based data analysis in Japan.\",\"authors\":\"Yuki Kimura, Hiroshi Ohtsu, Naohiro Yonemoto, Nobuyoshi Azuma, Kazuhiro Sase\",\"doi\":\"10.1136/bmjsit-2022-000131\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Endovascular aortic repair (EVAR) evolved through competition with open aortic repair (OAR) as a safe and effective treatment option for appropriately selected patients with abdominal aortic aneurysm (AAA). Although endoleaks are the most common reason for post-EVAR reintervention, compliance with lifelong regular follow-up imaging remains a challenge.</p><p><strong>Design: </strong>Retrospective data analysis.</p><p><strong>Setting: </strong>The Japan Medical Data Center (JMDC), a claims database with anonymous data linkage across hospitals, consists of corporate employees and their families of ≤75 years of age.</p><p><strong>Participants: </strong>The analysis included participants in the JMDC who underwent EVAR or OAR for intact (iAAA) or ruptured (rAAA) AAA. Patients with less than 6 months of records before the aortic repair were excluded.</p><p><strong>Main outcome measures: </strong>Overall survival and reintervention rates.</p><p><strong>Results: </strong>We identified 986 cases (837 iAAA and 149 rAAA) from JMDC with first aortic repairs between January 2015 and December 2020. The number of patients, median age (years (IQR)), follow-up (months) and post-procedure CT scan (times per year) were as follows: iAAA (OAR: n=593, 62.0 (57.0-67.0), 26.0, 1.6, EVAR: n=244, 65.0 (31.0-69.0), 17.0, 2.2), rAAA (OAR: n=110, 59.0 (53.0-59.0), 16.0, 2.1, EVAR: n=39, 62.0 (31.0-67.0), 18.0, 2.4). Reintervention rate was significantly higher among EVAR than OAR in rAAA (15.4% vs 8.2%, p=0.04). In iAAA, there were no group difference after 5 years (7.8% vs 11.0%, p=0.28), even though EVAR had initial advantage. There were no differences in mortality rate between EVAR and OAR for either rAAA or iAAA.</p><p><strong>Conclusions: </strong>Claims-based analysis in Japan showed no statistically significant difference in 5-year survival rates of the OAR and EVAR groups. However, the reintervention rate of EVAR in rAAA was significantly higher, suggesting the need for regular post-EVAR follow-up with imaging. Therefore, international collaborations for long-term outcome studies with real-world data are warranted.</p>\",\"PeriodicalId\":33349,\"journal\":{\"name\":\"BMJ Surgery Interventions Health Technologies\",\"volume\":\" \",\"pages\":\"e000131\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2022-07-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/31/5d/bmjsit-2022-000131.PMC9345055.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Surgery Interventions Health Technologies\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjsit-2022-000131\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Surgery Interventions Health Technologies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjsit-2022-000131","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
Endovascular versus open repair in patients with abdominal aortic aneurysm: a claims-based data analysis in Japan.
Objectives: Endovascular aortic repair (EVAR) evolved through competition with open aortic repair (OAR) as a safe and effective treatment option for appropriately selected patients with abdominal aortic aneurysm (AAA). Although endoleaks are the most common reason for post-EVAR reintervention, compliance with lifelong regular follow-up imaging remains a challenge.
Design: Retrospective data analysis.
Setting: The Japan Medical Data Center (JMDC), a claims database with anonymous data linkage across hospitals, consists of corporate employees and their families of ≤75 years of age.
Participants: The analysis included participants in the JMDC who underwent EVAR or OAR for intact (iAAA) or ruptured (rAAA) AAA. Patients with less than 6 months of records before the aortic repair were excluded.
Main outcome measures: Overall survival and reintervention rates.
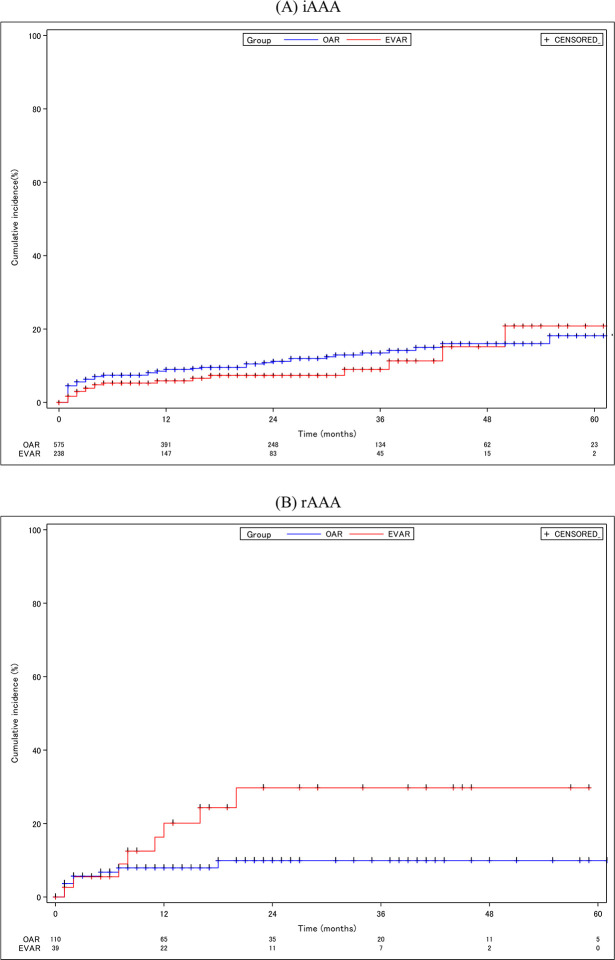
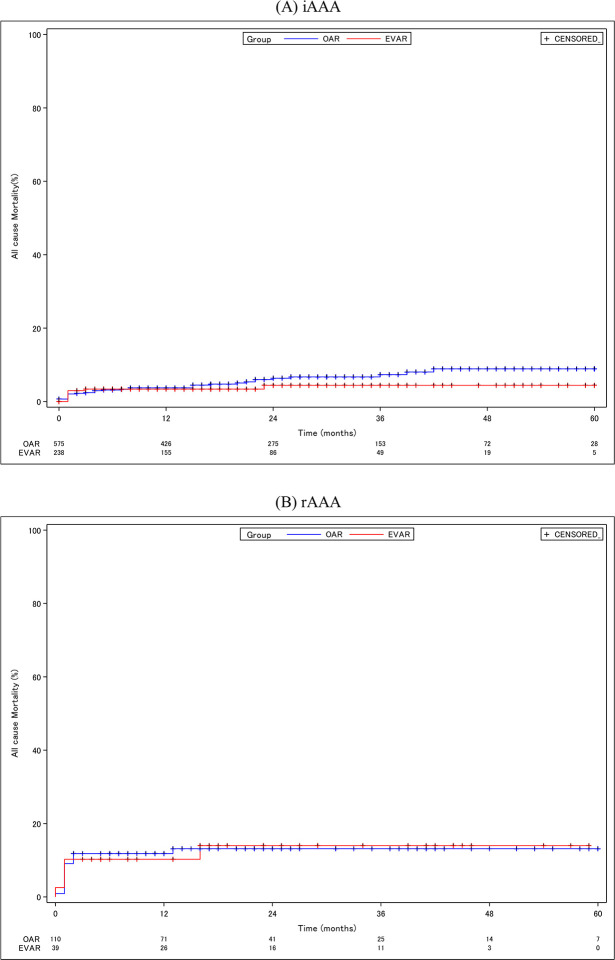
Results: We identified 986 cases (837 iAAA and 149 rAAA) from JMDC with first aortic repairs between January 2015 and December 2020. The number of patients, median age (years (IQR)), follow-up (months) and post-procedure CT scan (times per year) were as follows: iAAA (OAR: n=593, 62.0 (57.0-67.0), 26.0, 1.6, EVAR: n=244, 65.0 (31.0-69.0), 17.0, 2.2), rAAA (OAR: n=110, 59.0 (53.0-59.0), 16.0, 2.1, EVAR: n=39, 62.0 (31.0-67.0), 18.0, 2.4). Reintervention rate was significantly higher among EVAR than OAR in rAAA (15.4% vs 8.2%, p=0.04). In iAAA, there were no group difference after 5 years (7.8% vs 11.0%, p=0.28), even though EVAR had initial advantage. There were no differences in mortality rate between EVAR and OAR for either rAAA or iAAA.
Conclusions: Claims-based analysis in Japan showed no statistically significant difference in 5-year survival rates of the OAR and EVAR groups. However, the reintervention rate of EVAR in rAAA was significantly higher, suggesting the need for regular post-EVAR follow-up with imaging. Therefore, international collaborations for long-term outcome studies with real-world data are warranted.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


