{"title":"黄斑裂孔玻璃体切除术后视网膜脱离自行消退一例报告。","authors":"Seok Hyun Bae, Se Joon Woo","doi":"10.3341/kjo.2022.0030","DOIUrl":null,"url":null,"abstract":"Dear Editor, Retinal detachment (RD) after vitrectomy for macular hole can occur as a complication, either intraoperatively or postoperatively [1]. Iatrogenic retinal breaks are the most common cause, and many studies have described iatrogenic retinal breaks after macular hole surgery [1-3]. However, we encountered a case of RD that occurred after vitrectomy for macular hole, but a spontaneous reattachment occurred without further surgery. Thus, we would like to report this case. Written informed consent was obtained from the patient. A 72-year-old male patient was referred for evaluation because of decreased visual acuity in his right eye over 3 months. His best-corrected visual acuity was 20 / 125 (-1.75 0.75 × 85°) in the right eye and 20 / 20 (-0.75 0.75 × 75°) in the left eye. Intraocular pressure was 14 mmHg in the right eye and 16 mmHg in the left eye. The axial length of the eyes was 25.31 mm in the right eye and 25.18 mm in the left eye. He had no underlying diseases, such as diabetes or hypertension. Fundus examination and spectral domain optical coherence tomography showed a stage 3 full-thickness macular hole in the right eye and vitreomacular traction in the left eye without posterior staphyloma in both eyes (Fig. 1A). The patient underwent phacoemulsification and implantation of a posterior chamber intraocular lens, 25G pars plana vitrectomy, internal limiting membrane peeling, laser photocoagulation, and intravitreal gas tamponade (sulfur hexafluoride, 18%). There were no intraoperative complications. The patient was instructed to maintain a prone or sitting position for 7 days. After 1 week, the fundus examination revealed inferior bullous RD with macula involvement (Fig. 1B, 1C). An additional 25G pars plana vitrectomy, intraretinal fluid drainage, laser photocoagulation, and tamponade with a longer acting gas (octaf luoropropane, 14%) was performed. Although careful scleral depression was performed during the surgery, no retinal breaks were found. Therefore, retinotomy was performed for internal drainage of subretinal fluid at the superonasal region of the retina. Two weeks after the second operation, as the gas was absorbed, the fundus examination revealed redetachment of the retina (Fig. 1D). We suggested that the patient underwent reoperation using silicone oil, but the patient refused further surgery. We decided to monitor the patient without any other treatment. Instead, as the patient stated that he frequently adopted the supine position during sleep early after surgery, he was advised to strictly adopt a prone or sitting position. The patient returned 1 month later. His vision improved to 20 / 100. Although the macular hole remained, the RD subsided spontaneously (Fig. 1E, 1F). A final follow-up examination was performed 6 months after the last surgery. At this examination, no RD was observed, and the patient’s visual acuity was 20 / 125. This is the first case of spontaneous reattachment of RD that occurred after two vitrectomy surgeries for macular hole and RD. The most common cause of RD after macular hole surgery is a retinal break [1,3,4]. However, in our case, a retinal break was not observed, even though the retina was carefully indented during the operation. Another possible cause of RD after macular hole surgery Korean J Ophthalmol 2022;36(5):463-465 https://doi.org/10.3341/kjo.2022.0030","PeriodicalId":17883,"journal":{"name":"Korean Journal of Ophthalmology : KJO","volume":" ","pages":"463-465"},"PeriodicalIF":0.0000,"publicationDate":"2022-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/16/1f/kjo-2022-0030.PMC9582500.pdf","citationCount":"0","resultStr":"{\"title\":\"Spontaneous Resolution of Retinal Detachment that Occurred Following Vitrectomy for Macular Hole: A Case Report.\",\"authors\":\"Seok Hyun Bae, Se Joon Woo\",\"doi\":\"10.3341/kjo.2022.0030\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Dear Editor, Retinal detachment (RD) after vitrectomy for macular hole can occur as a complication, either intraoperatively or postoperatively [1]. Iatrogenic retinal breaks are the most common cause, and many studies have described iatrogenic retinal breaks after macular hole surgery [1-3]. However, we encountered a case of RD that occurred after vitrectomy for macular hole, but a spontaneous reattachment occurred without further surgery. Thus, we would like to report this case. Written informed consent was obtained from the patient. A 72-year-old male patient was referred for evaluation because of decreased visual acuity in his right eye over 3 months. His best-corrected visual acuity was 20 / 125 (-1.75 0.75 × 85°) in the right eye and 20 / 20 (-0.75 0.75 × 75°) in the left eye. Intraocular pressure was 14 mmHg in the right eye and 16 mmHg in the left eye. The axial length of the eyes was 25.31 mm in the right eye and 25.18 mm in the left eye. He had no underlying diseases, such as diabetes or hypertension. Fundus examination and spectral domain optical coherence tomography showed a stage 3 full-thickness macular hole in the right eye and vitreomacular traction in the left eye without posterior staphyloma in both eyes (Fig. 1A). The patient underwent phacoemulsification and implantation of a posterior chamber intraocular lens, 25G pars plana vitrectomy, internal limiting membrane peeling, laser photocoagulation, and intravitreal gas tamponade (sulfur hexafluoride, 18%). There were no intraoperative complications. The patient was instructed to maintain a prone or sitting position for 7 days. After 1 week, the fundus examination revealed inferior bullous RD with macula involvement (Fig. 1B, 1C). An additional 25G pars plana vitrectomy, intraretinal fluid drainage, laser photocoagulation, and tamponade with a longer acting gas (octaf luoropropane, 14%) was performed. Although careful scleral depression was performed during the surgery, no retinal breaks were found. Therefore, retinotomy was performed for internal drainage of subretinal fluid at the superonasal region of the retina. Two weeks after the second operation, as the gas was absorbed, the fundus examination revealed redetachment of the retina (Fig. 1D). We suggested that the patient underwent reoperation using silicone oil, but the patient refused further surgery. We decided to monitor the patient without any other treatment. Instead, as the patient stated that he frequently adopted the supine position during sleep early after surgery, he was advised to strictly adopt a prone or sitting position. The patient returned 1 month later. His vision improved to 20 / 100. Although the macular hole remained, the RD subsided spontaneously (Fig. 1E, 1F). A final follow-up examination was performed 6 months after the last surgery. At this examination, no RD was observed, and the patient’s visual acuity was 20 / 125. This is the first case of spontaneous reattachment of RD that occurred after two vitrectomy surgeries for macular hole and RD. The most common cause of RD after macular hole surgery is a retinal break [1,3,4]. However, in our case, a retinal break was not observed, even though the retina was carefully indented during the operation. Another possible cause of RD after macular hole surgery Korean J Ophthalmol 2022;36(5):463-465 https://doi.org/10.3341/kjo.2022.0030\",\"PeriodicalId\":17883,\"journal\":{\"name\":\"Korean Journal of Ophthalmology : KJO\",\"volume\":\" \",\"pages\":\"463-465\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/16/1f/kjo-2022-0030.PMC9582500.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Korean Journal of Ophthalmology : KJO\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3341/kjo.2022.0030\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/8/19 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Ophthalmology : KJO","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3341/kjo.2022.0030","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/8/19 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
Spontaneous Resolution of Retinal Detachment that Occurred Following Vitrectomy for Macular Hole: A Case Report.
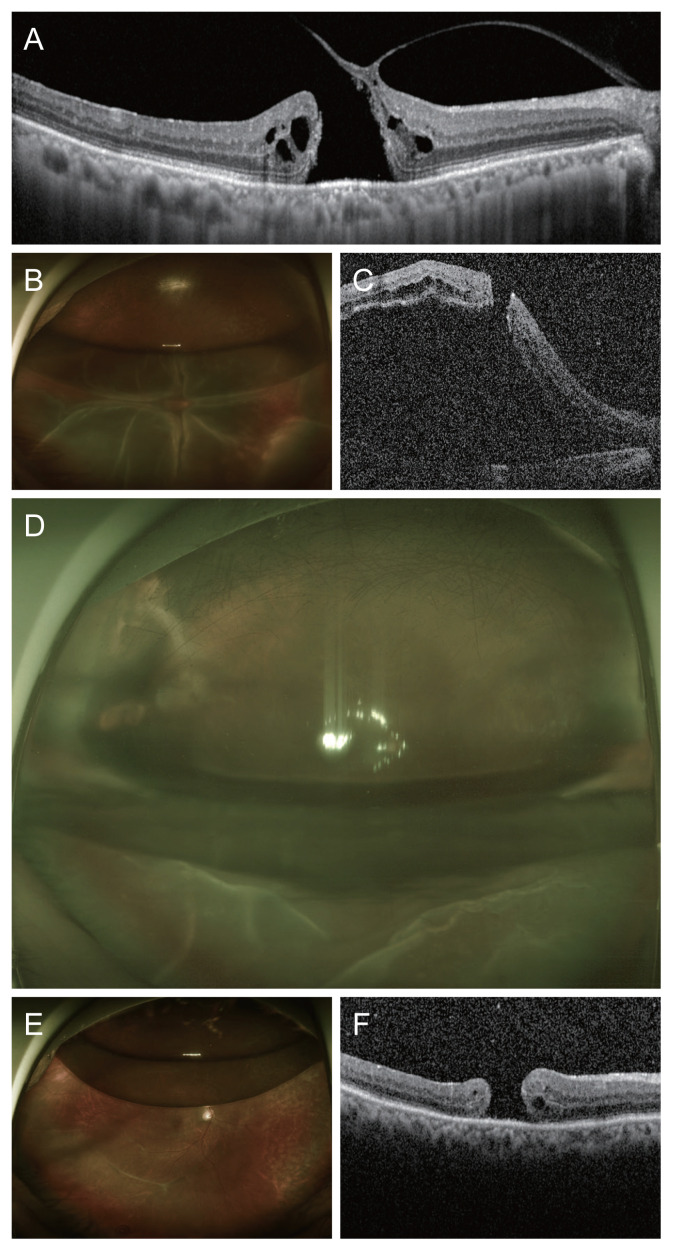
Dear Editor, Retinal detachment (RD) after vitrectomy for macular hole can occur as a complication, either intraoperatively or postoperatively [1]. Iatrogenic retinal breaks are the most common cause, and many studies have described iatrogenic retinal breaks after macular hole surgery [1-3]. However, we encountered a case of RD that occurred after vitrectomy for macular hole, but a spontaneous reattachment occurred without further surgery. Thus, we would like to report this case. Written informed consent was obtained from the patient. A 72-year-old male patient was referred for evaluation because of decreased visual acuity in his right eye over 3 months. His best-corrected visual acuity was 20 / 125 (-1.75 0.75 × 85°) in the right eye and 20 / 20 (-0.75 0.75 × 75°) in the left eye. Intraocular pressure was 14 mmHg in the right eye and 16 mmHg in the left eye. The axial length of the eyes was 25.31 mm in the right eye and 25.18 mm in the left eye. He had no underlying diseases, such as diabetes or hypertension. Fundus examination and spectral domain optical coherence tomography showed a stage 3 full-thickness macular hole in the right eye and vitreomacular traction in the left eye without posterior staphyloma in both eyes (Fig. 1A). The patient underwent phacoemulsification and implantation of a posterior chamber intraocular lens, 25G pars plana vitrectomy, internal limiting membrane peeling, laser photocoagulation, and intravitreal gas tamponade (sulfur hexafluoride, 18%). There were no intraoperative complications. The patient was instructed to maintain a prone or sitting position for 7 days. After 1 week, the fundus examination revealed inferior bullous RD with macula involvement (Fig. 1B, 1C). An additional 25G pars plana vitrectomy, intraretinal fluid drainage, laser photocoagulation, and tamponade with a longer acting gas (octaf luoropropane, 14%) was performed. Although careful scleral depression was performed during the surgery, no retinal breaks were found. Therefore, retinotomy was performed for internal drainage of subretinal fluid at the superonasal region of the retina. Two weeks after the second operation, as the gas was absorbed, the fundus examination revealed redetachment of the retina (Fig. 1D). We suggested that the patient underwent reoperation using silicone oil, but the patient refused further surgery. We decided to monitor the patient without any other treatment. Instead, as the patient stated that he frequently adopted the supine position during sleep early after surgery, he was advised to strictly adopt a prone or sitting position. The patient returned 1 month later. His vision improved to 20 / 100. Although the macular hole remained, the RD subsided spontaneously (Fig. 1E, 1F). A final follow-up examination was performed 6 months after the last surgery. At this examination, no RD was observed, and the patient’s visual acuity was 20 / 125. This is the first case of spontaneous reattachment of RD that occurred after two vitrectomy surgeries for macular hole and RD. The most common cause of RD after macular hole surgery is a retinal break [1,3,4]. However, in our case, a retinal break was not observed, even though the retina was carefully indented during the operation. Another possible cause of RD after macular hole surgery Korean J Ophthalmol 2022;36(5):463-465 https://doi.org/10.3341/kjo.2022.0030

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


