Mandar Koranne, Pratik D Patil, Suchin S Dhamnaskar
{"title":"外科医生在对COVID-19阳性患者进行手术时感染COVID-19的风险,安全措施的影响:经验教训。","authors":"Mandar Koranne, Pratik D Patil, Suchin S Dhamnaskar","doi":"10.1055/s-0042-1755619","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction</b> On March 11, 2020, the novel coronavirus disease 2019 (COVID-19) was declared as a pandemic. General surgeons provide care to COVID-19 positive patients requiring emergency surgeries and hence are exposed to the virus. Surgery on COVID-19-positive patient itself is a major risk factor for surgeon to contract COVID-19 infection. Noticeably, there is no data regarding number of surgeons who have contracted COVID-19 after operating on COVID-19-positive patients. Hence, the aim of this study was to find out the exact incidence of COVID-19 among surgeons operating on COVID-19-positive patients and to analyze the impact of safety measures practiced by us. <b>Methodology</b> The study was conducted in a tertiary care center in Mumbai. It was a retrospective observational study with duration of 5 months from May 1, 2020, to September 30, 2020. Only those surgeons (faculty and resident doctors) were included who performed surgeries on COVID-19-positive patients (diagnosed by reverse-transcription polymerase chain reaction [RT-PCR] test) and gave consent for participation. As an institutional protocol, all patients undergoing surgery were tested by RT-PCR test (irrespective of chest X-ray or symptoms). Nasopharyngeal swabs for COVID-19 disease were collected prior to procedure but in some of these, results came after surgery. Still such patients were included in this study. Irrespective of COVID-19 status, same precautions were taken for all surgeries. The details of the patients like date of surgery, age, sex, surgery performed, duration of surgery, type of anesthesia used, and operating surgeon were noted from operation room (OR) register. Details of surgeons (faculty and resident doctors) who fulfilled inclusion criteria were noted by interview in terms of their demographic parameters, such as age, sex, designation, experience in years after completing postgraduation, comorbidities, whether they ever contracted COVID-19 (if yes, date), and safety measures practiced (yes, no, or cannot recollect). Patient was assumed to be the source only if the surgeon contracted COVID-19 within 14 days of surgery. <b>Results</b> A total of 34 surgeons (7 faculty and 27 residents) conducted 41 surgeries on COVID-19-positive patients during the study period. All of them gave consent for participation in the study. More than one surgeon was involved in a particular surgery. Hence, there were 78 occasions (faculty during 16 occasions and resident doctors on 62 occasions) when surgeons were at risk to contract COVID-19 while operating on patients ( <i>n</i> = 78). These surgeries had similar/comparable risk of COVID-19 exposure to surgeons and procedures with excessive exposure risk like airway procedures did not happen during the study period. The mean age of surgeon was 27.92 years ( <i>n</i> = 78, standard deviation = 5.71) and median experience of faculty after completion of postgraduate degree was 7 years ( <i>n</i> = 16, interquartile range [IQR] = 1.25-11.0). Only one faculty had comorbidity (diabetes mellitus). Duration of surgeries ranged from 50 to 420 minutes with median being 190 minutes ( <i>n</i> = 41, IQR = 120-240). Only one surgeon (male faculty) contracted COVID-19 within 14 days of surgery (1.3% incidence, <i>n</i> = 78), a total of seven surgeons contracted COVID-19 during study period but not within 14 days of surgery (source other than patient operated) and all remaining surgeons were asymptomatic throughout the study period. The surgeon who contracted COVID-19 (within 14 days) performed surgery for 260 minutes and under general anesthesia. All the surgeons followed standard steps of donning and doffing, used personal protective equipment (PPE) body cover, shoe cover, hood, double pair of gloves, and N-95 masks at all times ( <i>n</i> = 78). Intubation box was used in 100% cases of general anesthesia ( <i>n</i> = 19). Fogging of OR after each surgery and interval of 20 minutes between surgeries was followed in 100% cases. Also, patient was wearing mask at all possible times and anesthetist and support staff used PPE during all surgeries. Hence the relationship between COVID-19 status and these safety measures cannot be assessed. Goggles and face shields were not used on 88.5% ( <i>n</i> = 78) and 93.2% ( <i>n</i> = 73, because five surgeons could not recollect whether they used face shields or not) occasions, respectively. Also, immediate shower after surgery was not taken on 93.6% occasions ( <i>n</i> = 78). The surgeon who contracted COVID-19 had neither used goggles nor face shield. Also, he did not take shower immediately after surgery. However, there was no significant association between use of goggles, face shields, or shower after surgery and contraction of COVID-19 after operating patients (Fisher's exact <i>p</i> = 1.000). Air conditioner was switched-off only in 7.3% surgeries ( <i>n</i> = 41). Smoke evacuator (cautery with attached suction) was not used in 97.6% cases. Clinical documentation (handling of patient's files) was done outside OR in only 17.1% surgeries ( <i>n</i> = 41). However, there was no significant association between these safety measures and contraction of COVID-19 (Fisher's exact <i>p</i> = 1.000). General anesthesia was used in 19 surgeries (46.3%) while spinal anesthesia in 16 surgeries (39%), local anesthesia in 5 surgeries (12.2%), and total intravenous anesthesia (TIVA) in one surgery (2.4%). However, there was no significant association between type of anesthesia given during surgery and contraction of COVID-19 after operating on patients with Fisher's exact <i>p</i> -value of 1.000. <b>Conclusion</b> Even though safety measures, like goggles, face shield, switching-off of air conditioner, use of smoke evacuator, and shower, immediately after surgery were not practiced in majority of cases, surgeon positivity rate was significantly less. Also, there was no use of negative pressure in OR. Hence, their significance becomes questionable. Although adopting all universal safety measures is in everyone's best interest, it is seldom cost-effective. To reduce resource exhaustion, especially in a pandemic situation, the use of various safety measures and staff must be balanced. Use and promotion of unnecessary safety measures leads to added health care costs and fear among health care workers in case of unavailability. Even though our study has a small sample size and has its own limitations, it can guide future studies to strengthen recommendations and reduce health care costs. This will also help in future epidemics/pandemics.</p>","PeriodicalId":44614,"journal":{"name":"Surgery Journal","volume":" ","pages":"e192-e198"},"PeriodicalIF":0.8000,"publicationDate":"2022-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9395240/pdf/","citationCount":"1","resultStr":"{\"title\":\"Risk of Surgeon Contracting COVID-19 while Operating on COVID-19-Positive Patient, Impact of Safety Measures: Lessons Learnt.\",\"authors\":\"Mandar Koranne, Pratik D Patil, Suchin S Dhamnaskar\",\"doi\":\"10.1055/s-0042-1755619\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Introduction</b> On March 11, 2020, the novel coronavirus disease 2019 (COVID-19) was declared as a pandemic. General surgeons provide care to COVID-19 positive patients requiring emergency surgeries and hence are exposed to the virus. Surgery on COVID-19-positive patient itself is a major risk factor for surgeon to contract COVID-19 infection. Noticeably, there is no data regarding number of surgeons who have contracted COVID-19 after operating on COVID-19-positive patients. Hence, the aim of this study was to find out the exact incidence of COVID-19 among surgeons operating on COVID-19-positive patients and to analyze the impact of safety measures practiced by us. <b>Methodology</b> The study was conducted in a tertiary care center in Mumbai. It was a retrospective observational study with duration of 5 months from May 1, 2020, to September 30, 2020. Only those surgeons (faculty and resident doctors) were included who performed surgeries on COVID-19-positive patients (diagnosed by reverse-transcription polymerase chain reaction [RT-PCR] test) and gave consent for participation. As an institutional protocol, all patients undergoing surgery were tested by RT-PCR test (irrespective of chest X-ray or symptoms). Nasopharyngeal swabs for COVID-19 disease were collected prior to procedure but in some of these, results came after surgery. Still such patients were included in this study. Irrespective of COVID-19 status, same precautions were taken for all surgeries. The details of the patients like date of surgery, age, sex, surgery performed, duration of surgery, type of anesthesia used, and operating surgeon were noted from operation room (OR) register. Details of surgeons (faculty and resident doctors) who fulfilled inclusion criteria were noted by interview in terms of their demographic parameters, such as age, sex, designation, experience in years after completing postgraduation, comorbidities, whether they ever contracted COVID-19 (if yes, date), and safety measures practiced (yes, no, or cannot recollect). Patient was assumed to be the source only if the surgeon contracted COVID-19 within 14 days of surgery. <b>Results</b> A total of 34 surgeons (7 faculty and 27 residents) conducted 41 surgeries on COVID-19-positive patients during the study period. All of them gave consent for participation in the study. More than one surgeon was involved in a particular surgery. Hence, there were 78 occasions (faculty during 16 occasions and resident doctors on 62 occasions) when surgeons were at risk to contract COVID-19 while operating on patients ( <i>n</i> = 78). These surgeries had similar/comparable risk of COVID-19 exposure to surgeons and procedures with excessive exposure risk like airway procedures did not happen during the study period. The mean age of surgeon was 27.92 years ( <i>n</i> = 78, standard deviation = 5.71) and median experience of faculty after completion of postgraduate degree was 7 years ( <i>n</i> = 16, interquartile range [IQR] = 1.25-11.0). Only one faculty had comorbidity (diabetes mellitus). Duration of surgeries ranged from 50 to 420 minutes with median being 190 minutes ( <i>n</i> = 41, IQR = 120-240). Only one surgeon (male faculty) contracted COVID-19 within 14 days of surgery (1.3% incidence, <i>n</i> = 78), a total of seven surgeons contracted COVID-19 during study period but not within 14 days of surgery (source other than patient operated) and all remaining surgeons were asymptomatic throughout the study period. The surgeon who contracted COVID-19 (within 14 days) performed surgery for 260 minutes and under general anesthesia. All the surgeons followed standard steps of donning and doffing, used personal protective equipment (PPE) body cover, shoe cover, hood, double pair of gloves, and N-95 masks at all times ( <i>n</i> = 78). Intubation box was used in 100% cases of general anesthesia ( <i>n</i> = 19). Fogging of OR after each surgery and interval of 20 minutes between surgeries was followed in 100% cases. Also, patient was wearing mask at all possible times and anesthetist and support staff used PPE during all surgeries. Hence the relationship between COVID-19 status and these safety measures cannot be assessed. Goggles and face shields were not used on 88.5% ( <i>n</i> = 78) and 93.2% ( <i>n</i> = 73, because five surgeons could not recollect whether they used face shields or not) occasions, respectively. Also, immediate shower after surgery was not taken on 93.6% occasions ( <i>n</i> = 78). The surgeon who contracted COVID-19 had neither used goggles nor face shield. Also, he did not take shower immediately after surgery. However, there was no significant association between use of goggles, face shields, or shower after surgery and contraction of COVID-19 after operating patients (Fisher's exact <i>p</i> = 1.000). Air conditioner was switched-off only in 7.3% surgeries ( <i>n</i> = 41). Smoke evacuator (cautery with attached suction) was not used in 97.6% cases. Clinical documentation (handling of patient's files) was done outside OR in only 17.1% surgeries ( <i>n</i> = 41). However, there was no significant association between these safety measures and contraction of COVID-19 (Fisher's exact <i>p</i> = 1.000). General anesthesia was used in 19 surgeries (46.3%) while spinal anesthesia in 16 surgeries (39%), local anesthesia in 5 surgeries (12.2%), and total intravenous anesthesia (TIVA) in one surgery (2.4%). However, there was no significant association between type of anesthesia given during surgery and contraction of COVID-19 after operating on patients with Fisher's exact <i>p</i> -value of 1.000. <b>Conclusion</b> Even though safety measures, like goggles, face shield, switching-off of air conditioner, use of smoke evacuator, and shower, immediately after surgery were not practiced in majority of cases, surgeon positivity rate was significantly less. Also, there was no use of negative pressure in OR. Hence, their significance becomes questionable. Although adopting all universal safety measures is in everyone's best interest, it is seldom cost-effective. To reduce resource exhaustion, especially in a pandemic situation, the use of various safety measures and staff must be balanced. Use and promotion of unnecessary safety measures leads to added health care costs and fear among health care workers in case of unavailability. Even though our study has a small sample size and has its own limitations, it can guide future studies to strengthen recommendations and reduce health care costs. This will also help in future epidemics/pandemics.</p>\",\"PeriodicalId\":44614,\"journal\":{\"name\":\"Surgery Journal\",\"volume\":\" \",\"pages\":\"e192-e198\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2022-08-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9395240/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Surgery Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/s-0042-1755619\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgery Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0042-1755619","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/7/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
Risk of Surgeon Contracting COVID-19 while Operating on COVID-19-Positive Patient, Impact of Safety Measures: Lessons Learnt.
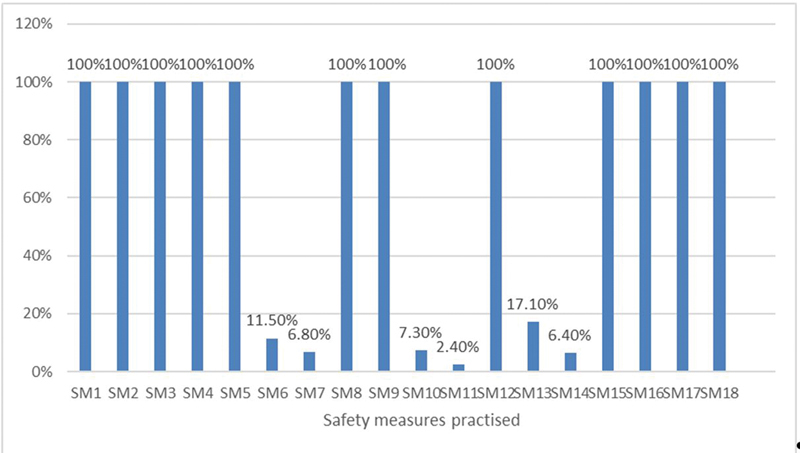
Introduction On March 11, 2020, the novel coronavirus disease 2019 (COVID-19) was declared as a pandemic. General surgeons provide care to COVID-19 positive patients requiring emergency surgeries and hence are exposed to the virus. Surgery on COVID-19-positive patient itself is a major risk factor for surgeon to contract COVID-19 infection. Noticeably, there is no data regarding number of surgeons who have contracted COVID-19 after operating on COVID-19-positive patients. Hence, the aim of this study was to find out the exact incidence of COVID-19 among surgeons operating on COVID-19-positive patients and to analyze the impact of safety measures practiced by us. Methodology The study was conducted in a tertiary care center in Mumbai. It was a retrospective observational study with duration of 5 months from May 1, 2020, to September 30, 2020. Only those surgeons (faculty and resident doctors) were included who performed surgeries on COVID-19-positive patients (diagnosed by reverse-transcription polymerase chain reaction [RT-PCR] test) and gave consent for participation. As an institutional protocol, all patients undergoing surgery were tested by RT-PCR test (irrespective of chest X-ray or symptoms). Nasopharyngeal swabs for COVID-19 disease were collected prior to procedure but in some of these, results came after surgery. Still such patients were included in this study. Irrespective of COVID-19 status, same precautions were taken for all surgeries. The details of the patients like date of surgery, age, sex, surgery performed, duration of surgery, type of anesthesia used, and operating surgeon were noted from operation room (OR) register. Details of surgeons (faculty and resident doctors) who fulfilled inclusion criteria were noted by interview in terms of their demographic parameters, such as age, sex, designation, experience in years after completing postgraduation, comorbidities, whether they ever contracted COVID-19 (if yes, date), and safety measures practiced (yes, no, or cannot recollect). Patient was assumed to be the source only if the surgeon contracted COVID-19 within 14 days of surgery. Results A total of 34 surgeons (7 faculty and 27 residents) conducted 41 surgeries on COVID-19-positive patients during the study period. All of them gave consent for participation in the study. More than one surgeon was involved in a particular surgery. Hence, there were 78 occasions (faculty during 16 occasions and resident doctors on 62 occasions) when surgeons were at risk to contract COVID-19 while operating on patients ( n = 78). These surgeries had similar/comparable risk of COVID-19 exposure to surgeons and procedures with excessive exposure risk like airway procedures did not happen during the study period. The mean age of surgeon was 27.92 years ( n = 78, standard deviation = 5.71) and median experience of faculty after completion of postgraduate degree was 7 years ( n = 16, interquartile range [IQR] = 1.25-11.0). Only one faculty had comorbidity (diabetes mellitus). Duration of surgeries ranged from 50 to 420 minutes with median being 190 minutes ( n = 41, IQR = 120-240). Only one surgeon (male faculty) contracted COVID-19 within 14 days of surgery (1.3% incidence, n = 78), a total of seven surgeons contracted COVID-19 during study period but not within 14 days of surgery (source other than patient operated) and all remaining surgeons were asymptomatic throughout the study period. The surgeon who contracted COVID-19 (within 14 days) performed surgery for 260 minutes and under general anesthesia. All the surgeons followed standard steps of donning and doffing, used personal protective equipment (PPE) body cover, shoe cover, hood, double pair of gloves, and N-95 masks at all times ( n = 78). Intubation box was used in 100% cases of general anesthesia ( n = 19). Fogging of OR after each surgery and interval of 20 minutes between surgeries was followed in 100% cases. Also, patient was wearing mask at all possible times and anesthetist and support staff used PPE during all surgeries. Hence the relationship between COVID-19 status and these safety measures cannot be assessed. Goggles and face shields were not used on 88.5% ( n = 78) and 93.2% ( n = 73, because five surgeons could not recollect whether they used face shields or not) occasions, respectively. Also, immediate shower after surgery was not taken on 93.6% occasions ( n = 78). The surgeon who contracted COVID-19 had neither used goggles nor face shield. Also, he did not take shower immediately after surgery. However, there was no significant association between use of goggles, face shields, or shower after surgery and contraction of COVID-19 after operating patients (Fisher's exact p = 1.000). Air conditioner was switched-off only in 7.3% surgeries ( n = 41). Smoke evacuator (cautery with attached suction) was not used in 97.6% cases. Clinical documentation (handling of patient's files) was done outside OR in only 17.1% surgeries ( n = 41). However, there was no significant association between these safety measures and contraction of COVID-19 (Fisher's exact p = 1.000). General anesthesia was used in 19 surgeries (46.3%) while spinal anesthesia in 16 surgeries (39%), local anesthesia in 5 surgeries (12.2%), and total intravenous anesthesia (TIVA) in one surgery (2.4%). However, there was no significant association between type of anesthesia given during surgery and contraction of COVID-19 after operating on patients with Fisher's exact p -value of 1.000. Conclusion Even though safety measures, like goggles, face shield, switching-off of air conditioner, use of smoke evacuator, and shower, immediately after surgery were not practiced in majority of cases, surgeon positivity rate was significantly less. Also, there was no use of negative pressure in OR. Hence, their significance becomes questionable. Although adopting all universal safety measures is in everyone's best interest, it is seldom cost-effective. To reduce resource exhaustion, especially in a pandemic situation, the use of various safety measures and staff must be balanced. Use and promotion of unnecessary safety measures leads to added health care costs and fear among health care workers in case of unavailability. Even though our study has a small sample size and has its own limitations, it can guide future studies to strengthen recommendations and reduce health care costs. This will also help in future epidemics/pandemics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


