Marie-Louise Bird, Felix Peel, Matt Schmidt, Natalie A Fini, Emily Ramage, Brodie M Sakakibara, Dawn B Simpson, Carey Mather, Dominique A Cadilhac, Kiran D K Ahuja, Heather Bridgman, Coralie English
{"title":"移动为重点的物理结果测量电信技术(变焦):内部和内部可靠性试验。","authors":"Marie-Louise Bird, Felix Peel, Matt Schmidt, Natalie A Fini, Emily Ramage, Brodie M Sakakibara, Dawn B Simpson, Carey Mather, Dominique A Cadilhac, Kiran D K Ahuja, Heather Bridgman, Coralie English","doi":"10.2196/38101","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Rehabilitation provided via telehealth offers an alternative to currently limited in-person health care. Effective rehabilitation depends on accurate and relevant assessments that reliably measure changes in function over time. The reliability of a suite of relevant assessments to measure the impact of rehabilitation on physical function is unknown.</p><p><strong>Objective: </strong>We aimed to measure the intrarater reliability of mobility-focused physical outcome measures delivered via Zoom (a commonly used telecommunication platform) and interrater reliability, comparing Zoom with in-person measures.</p><p><strong>Methods: </strong>In this reliability trial, healthy volunteers were recruited to complete 7 mobility-focused outcome measures in view of a laptop, under instructions from a remotely based researcher who undertook the remote evaluations. An in-person researcher (providing the benchmark scores) concurrently recorded their scores. Interrater and intrarater reliability were assessed for Grip Strength, Functional Reach Test, 5-Time Sit to Stand, 3- and 4-Meter Walks and Timed Up and Go, using intraclass correlation coefficients (ICC) and Bland-Altman plots. These tests were chosen because they cover a wide array of physical mobility, strength, and balance constructs; require little to no assistance from a clinician; can be performed in the limits of a home environment; and are likely to be feasible over a telehealth delivery mode.</p><p><strong>Results: </strong>A total of 30 participants (mean age 36.2, SD 12.5 years; n=19, 63% male) completed all assessments. Interrater reliability was excellent for Grip Strength (ICC=0.99) and Functional Reach Test (ICC=0.99), good for 5-Time Sit to Stand (ICC=0.842) and 4-Meter Walk (ICC=0.76), moderate for Timed Up and Go (ICC=0.64), and poor for 3-Meter Walk (ICC=-0.46). Intrarater reliability, accessed by the remote researcher, was excellent for Grip Strength (ICC=0.91); good for Timed Up and Go, 3-Meter Walk, 4-Meter Walk, and Functional Reach (ICC=0.84-0.89); and moderate for 5-Time Sit to Stand (ICC=0.67). Although recorded simultaneously, the following time-based assessments were recorded as significantly longer via Zoom: 5-Time Sit to Stand (1.2 seconds), Timed Up and Go (1.0 seconds), and 3-Meter Walk (1.3 seconds).</p><p><strong>Conclusions: </strong>Untimed mobility-focused physical outcome measures have excellent interrater reliability between in-person and telehealth measurements. Timed outcome measures took approximately 1 second longer via Zoom, reducing the reliability of tests with a shorter duration. Small time differences favoring in-person attendance are of a similar magnitude to clinically important differences, indicating assessments undertaken using telecommunications technology (Zoom) cannot be compared directly with face-to-face delivery. This has implications for clinicians using blended (ie, some face-to-face and some via the internet) assessments. High intrarater reliability of mobility-focused physical outcome measures has been demonstrated in this study.</p>","PeriodicalId":36224,"journal":{"name":"JMIR Rehabilitation and Assistive Technologies","volume":" ","pages":"e38101"},"PeriodicalIF":0.0000,"publicationDate":"2022-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9446136/pdf/","citationCount":"0","resultStr":"{\"title\":\"Mobility-Focused Physical Outcome Measures Over Telecommunication Technology (Zoom): Intra and Interrater Reliability Trial.\",\"authors\":\"Marie-Louise Bird, Felix Peel, Matt Schmidt, Natalie A Fini, Emily Ramage, Brodie M Sakakibara, Dawn B Simpson, Carey Mather, Dominique A Cadilhac, Kiran D K Ahuja, Heather Bridgman, Coralie English\",\"doi\":\"10.2196/38101\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Rehabilitation provided via telehealth offers an alternative to currently limited in-person health care. Effective rehabilitation depends on accurate and relevant assessments that reliably measure changes in function over time. The reliability of a suite of relevant assessments to measure the impact of rehabilitation on physical function is unknown.</p><p><strong>Objective: </strong>We aimed to measure the intrarater reliability of mobility-focused physical outcome measures delivered via Zoom (a commonly used telecommunication platform) and interrater reliability, comparing Zoom with in-person measures.</p><p><strong>Methods: </strong>In this reliability trial, healthy volunteers were recruited to complete 7 mobility-focused outcome measures in view of a laptop, under instructions from a remotely based researcher who undertook the remote evaluations. An in-person researcher (providing the benchmark scores) concurrently recorded their scores. Interrater and intrarater reliability were assessed for Grip Strength, Functional Reach Test, 5-Time Sit to Stand, 3- and 4-Meter Walks and Timed Up and Go, using intraclass correlation coefficients (ICC) and Bland-Altman plots. These tests were chosen because they cover a wide array of physical mobility, strength, and balance constructs; require little to no assistance from a clinician; can be performed in the limits of a home environment; and are likely to be feasible over a telehealth delivery mode.</p><p><strong>Results: </strong>A total of 30 participants (mean age 36.2, SD 12.5 years; n=19, 63% male) completed all assessments. Interrater reliability was excellent for Grip Strength (ICC=0.99) and Functional Reach Test (ICC=0.99), good for 5-Time Sit to Stand (ICC=0.842) and 4-Meter Walk (ICC=0.76), moderate for Timed Up and Go (ICC=0.64), and poor for 3-Meter Walk (ICC=-0.46). Intrarater reliability, accessed by the remote researcher, was excellent for Grip Strength (ICC=0.91); good for Timed Up and Go, 3-Meter Walk, 4-Meter Walk, and Functional Reach (ICC=0.84-0.89); and moderate for 5-Time Sit to Stand (ICC=0.67). Although recorded simultaneously, the following time-based assessments were recorded as significantly longer via Zoom: 5-Time Sit to Stand (1.2 seconds), Timed Up and Go (1.0 seconds), and 3-Meter Walk (1.3 seconds).</p><p><strong>Conclusions: </strong>Untimed mobility-focused physical outcome measures have excellent interrater reliability between in-person and telehealth measurements. Timed outcome measures took approximately 1 second longer via Zoom, reducing the reliability of tests with a shorter duration. Small time differences favoring in-person attendance are of a similar magnitude to clinically important differences, indicating assessments undertaken using telecommunications technology (Zoom) cannot be compared directly with face-to-face delivery. This has implications for clinicians using blended (ie, some face-to-face and some via the internet) assessments. High intrarater reliability of mobility-focused physical outcome measures has been demonstrated in this study.</p>\",\"PeriodicalId\":36224,\"journal\":{\"name\":\"JMIR Rehabilitation and Assistive Technologies\",\"volume\":\" \",\"pages\":\"e38101\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-08-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9446136/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JMIR Rehabilitation and Assistive Technologies\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2196/38101\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR Rehabilitation and Assistive Technologies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/38101","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
背景:通过远程保健提供的康复是目前有限的面对面保健的另一种选择。有效的康复取决于准确和相关的评估,可靠地测量功能随时间的变化。一套测量康复对身体功能影响的相关评估的可靠性尚不清楚。目的:我们旨在测量通过Zoom(一种常用的电信平台)提供的以移动为重点的物理结果测量的内部可靠性和内部可靠性,并将Zoom与面对面测量进行比较。方法:在这项可靠性试验中,招募健康志愿者在远程研究人员的指导下,通过笔记本电脑完成7项以活动为重点的结果测量。一名现场研究人员(提供基准分数)同时记录他们的分数。采用类内相关系数(ICC)和Bland-Altman图,评估了握力、功能伸展测试、5次坐立、3米和4米步行以及计时起身和行走的组间和组内信度。选择这些测试是因为它们涵盖了广泛的身体活动、力量和平衡结构;几乎不需要临床医生的帮助;可在有限的家庭环境中进行;并且可能在远程医疗交付模式上是可行的。结果:共有30名参与者(平均年龄36.2岁,SD 12.5岁;N =19(63%男性)完成了所有评估。在握力测试(ICC=0.99)和功能伸展测试(ICC=0.99)中,评分者的信度非常好,在5次坐立测试(ICC=0.842)和4米步行测试(ICC=0.76)中,评分者的信度中等(ICC=0.64),在3米步行测试(ICC=-0.46)中评分者的信度较差。远程研究人员访问的内部信度对握力非常好(ICC=0.91);适用于计时起跑、3米步行、4米步行和功能性伸展(ICC=0.84-0.89);中度为5次坐立(ICC=0.67)。虽然是同时记录的,但以下基于时间的评估通过Zoom记录的时间明显更长:5-Time坐到站(1.2秒),Timed Up and Go(1.0秒),以及3米步行(1.3秒)。结论:非定时的以移动为重点的身体结果测量在面对面和远程医疗测量之间具有出色的互信度。通过Zoom计时结果测量大约多花了1秒,降低了测试的可靠性,持续时间较短。有利于亲自就诊的小时间差异与临床重要差异的大小相似,表明使用电信技术(Zoom)进行的评估不能直接与面对面交付进行比较。这对临床医生使用混合评估(即,一些面对面和一些通过互联网)有影响。本研究证明了以活动为重点的身体结果测量的高内部可靠性。
Mobility-Focused Physical Outcome Measures Over Telecommunication Technology (Zoom): Intra and Interrater Reliability Trial.
Background: Rehabilitation provided via telehealth offers an alternative to currently limited in-person health care. Effective rehabilitation depends on accurate and relevant assessments that reliably measure changes in function over time. The reliability of a suite of relevant assessments to measure the impact of rehabilitation on physical function is unknown.
Objective: We aimed to measure the intrarater reliability of mobility-focused physical outcome measures delivered via Zoom (a commonly used telecommunication platform) and interrater reliability, comparing Zoom with in-person measures.
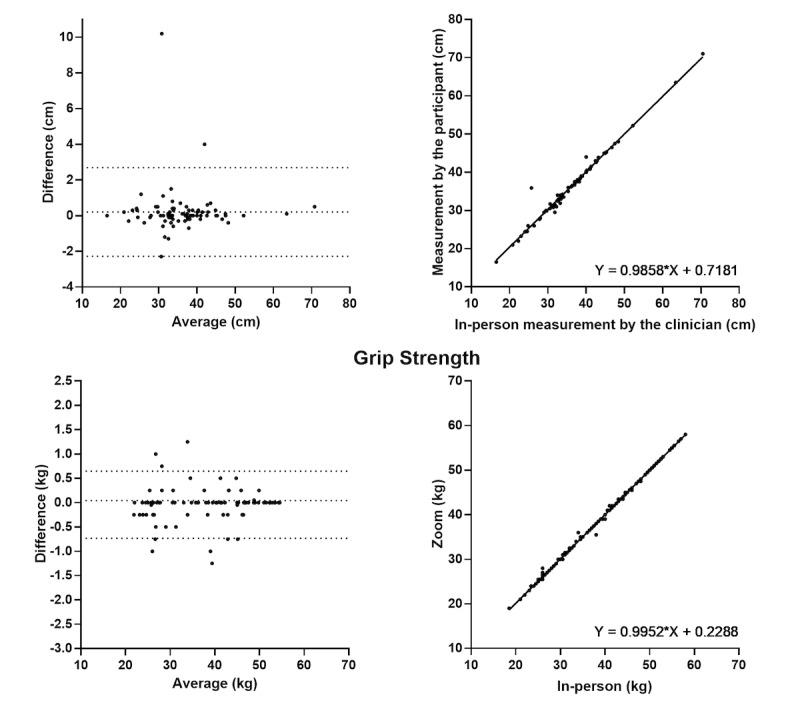
Methods: In this reliability trial, healthy volunteers were recruited to complete 7 mobility-focused outcome measures in view of a laptop, under instructions from a remotely based researcher who undertook the remote evaluations. An in-person researcher (providing the benchmark scores) concurrently recorded their scores. Interrater and intrarater reliability were assessed for Grip Strength, Functional Reach Test, 5-Time Sit to Stand, 3- and 4-Meter Walks and Timed Up and Go, using intraclass correlation coefficients (ICC) and Bland-Altman plots. These tests were chosen because they cover a wide array of physical mobility, strength, and balance constructs; require little to no assistance from a clinician; can be performed in the limits of a home environment; and are likely to be feasible over a telehealth delivery mode.
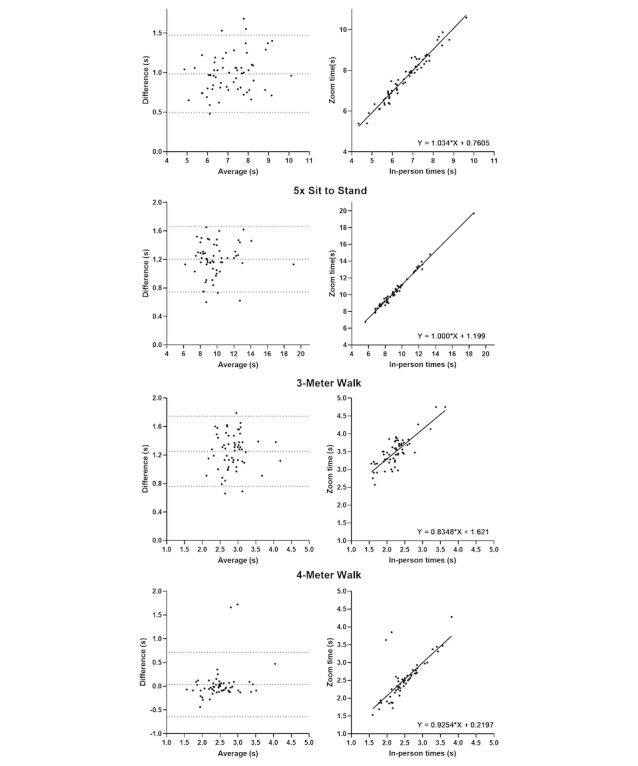
Results: A total of 30 participants (mean age 36.2, SD 12.5 years; n=19, 63% male) completed all assessments. Interrater reliability was excellent for Grip Strength (ICC=0.99) and Functional Reach Test (ICC=0.99), good for 5-Time Sit to Stand (ICC=0.842) and 4-Meter Walk (ICC=0.76), moderate for Timed Up and Go (ICC=0.64), and poor for 3-Meter Walk (ICC=-0.46). Intrarater reliability, accessed by the remote researcher, was excellent for Grip Strength (ICC=0.91); good for Timed Up and Go, 3-Meter Walk, 4-Meter Walk, and Functional Reach (ICC=0.84-0.89); and moderate for 5-Time Sit to Stand (ICC=0.67). Although recorded simultaneously, the following time-based assessments were recorded as significantly longer via Zoom: 5-Time Sit to Stand (1.2 seconds), Timed Up and Go (1.0 seconds), and 3-Meter Walk (1.3 seconds).
Conclusions: Untimed mobility-focused physical outcome measures have excellent interrater reliability between in-person and telehealth measurements. Timed outcome measures took approximately 1 second longer via Zoom, reducing the reliability of tests with a shorter duration. Small time differences favoring in-person attendance are of a similar magnitude to clinically important differences, indicating assessments undertaken using telecommunications technology (Zoom) cannot be compared directly with face-to-face delivery. This has implications for clinicians using blended (ie, some face-to-face and some via the internet) assessments. High intrarater reliability of mobility-focused physical outcome measures has been demonstrated in this study.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


