{"title":"加速预处理评估对丙型肝炎感染者注射毒品与护理联系的影响","authors":"Valérie Martel-Laferrière, Suzanne Brissette, Claire Wartelle-Bladou, Louis-Christophe Juteau, Maria Popa, Marie-Ève Goyer, Julie Bruneau","doi":"10.1177/11782218221119068","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Historically, hepatitis C virus (HCV) pretreatment evaluation has required multiple visits, frequently resulting in loss to follow-up and a delayed initiation of treatment. New technologies can accelerate this process. We investigated the feasibility of a single-day evaluation program and its impact on evaluation completion, treatment eligibility awareness, and treatment initiation among people who inject drugs (PWIDs).</p><p><strong>Methods: </strong>HCV-infected PWID who were unaware if they were eligible for treatment were recruited in a prospective evaluation of an accelerated model of care between 2017 and 2019 and compared to a historical cohort. The patients underwent a medical evaluation, rapid HCV viral load testing, and transient elastography during a single visit, at the end of which they were informed whether they were eligible for treatment. A historical cohort of patients fulfilling the same inclusion criteria and evaluated with the usual standard of care spanning several visits who were examined at the addiction medicine clinic from 2014 to 2016 served as the comparison group.</p><p><strong>Results: </strong>The accelerated and historical cohorts included 99 and 76 patients, respectively. The cohorts did not differ significantly by age and gender, but more patients in the historical cohort were undergoing opioid agonist therapy, while more patients in the accelerated cohort injected drugs in the last month. An accelerated evaluation resulted in a higher rate of evaluation completion (100% vs 67.1%; <i>P</i> < .001). Among those eligible for treatment, the proportion of those initiating treatment was similar between the groups (51/64 (79.7%) vs. 26/37 (70.3%); <i>P</i> = .28). The delay in the initiation of treatment was shorter in the accelerated cohort than in the historical cohort (69 (IQR: 49-106) days vs. 219 (IQR: 141-416) days; <i>P</i> < .001).</p><p><strong>Conclusions: </strong>Accelerated evaluation enhanced the awareness of eligibility and reduced the time to initiation among eligible patients.</p><p><strong>Trial registration: </strong>This study is registered on www.clinicaltrials.gov (NCT02755402).</p>","PeriodicalId":22185,"journal":{"name":"Substance Abuse: Research and Treatment","volume":" ","pages":"11782218221119068"},"PeriodicalIF":2.4000,"publicationDate":"2022-08-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/15/20/10.1177_11782218221119068.PMC9382068.pdf","citationCount":"1","resultStr":"{\"title\":\"Impact of an Accelerated Pretreatment Evaluation on Linkage-to-Care for Hepatitis C-infected Persons Who Inject Drugs.\",\"authors\":\"Valérie Martel-Laferrière, Suzanne Brissette, Claire Wartelle-Bladou, Louis-Christophe Juteau, Maria Popa, Marie-Ève Goyer, Julie Bruneau\",\"doi\":\"10.1177/11782218221119068\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Historically, hepatitis C virus (HCV) pretreatment evaluation has required multiple visits, frequently resulting in loss to follow-up and a delayed initiation of treatment. New technologies can accelerate this process. We investigated the feasibility of a single-day evaluation program and its impact on evaluation completion, treatment eligibility awareness, and treatment initiation among people who inject drugs (PWIDs).</p><p><strong>Methods: </strong>HCV-infected PWID who were unaware if they were eligible for treatment were recruited in a prospective evaluation of an accelerated model of care between 2017 and 2019 and compared to a historical cohort. The patients underwent a medical evaluation, rapid HCV viral load testing, and transient elastography during a single visit, at the end of which they were informed whether they were eligible for treatment. A historical cohort of patients fulfilling the same inclusion criteria and evaluated with the usual standard of care spanning several visits who were examined at the addiction medicine clinic from 2014 to 2016 served as the comparison group.</p><p><strong>Results: </strong>The accelerated and historical cohorts included 99 and 76 patients, respectively. The cohorts did not differ significantly by age and gender, but more patients in the historical cohort were undergoing opioid agonist therapy, while more patients in the accelerated cohort injected drugs in the last month. An accelerated evaluation resulted in a higher rate of evaluation completion (100% vs 67.1%; <i>P</i> < .001). Among those eligible for treatment, the proportion of those initiating treatment was similar between the groups (51/64 (79.7%) vs. 26/37 (70.3%); <i>P</i> = .28). The delay in the initiation of treatment was shorter in the accelerated cohort than in the historical cohort (69 (IQR: 49-106) days vs. 219 (IQR: 141-416) days; <i>P</i> < .001).</p><p><strong>Conclusions: </strong>Accelerated evaluation enhanced the awareness of eligibility and reduced the time to initiation among eligible patients.</p><p><strong>Trial registration: </strong>This study is registered on www.clinicaltrials.gov (NCT02755402).</p>\",\"PeriodicalId\":22185,\"journal\":{\"name\":\"Substance Abuse: Research and Treatment\",\"volume\":\" \",\"pages\":\"11782218221119068\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2022-08-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/15/20/10.1177_11782218221119068.PMC9382068.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Substance Abuse: Research and Treatment\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/11782218221119068\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"SUBSTANCE ABUSE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Substance Abuse: Research and Treatment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11782218221119068","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SUBSTANCE ABUSE","Score":null,"Total":0}
引用次数: 1
摘要
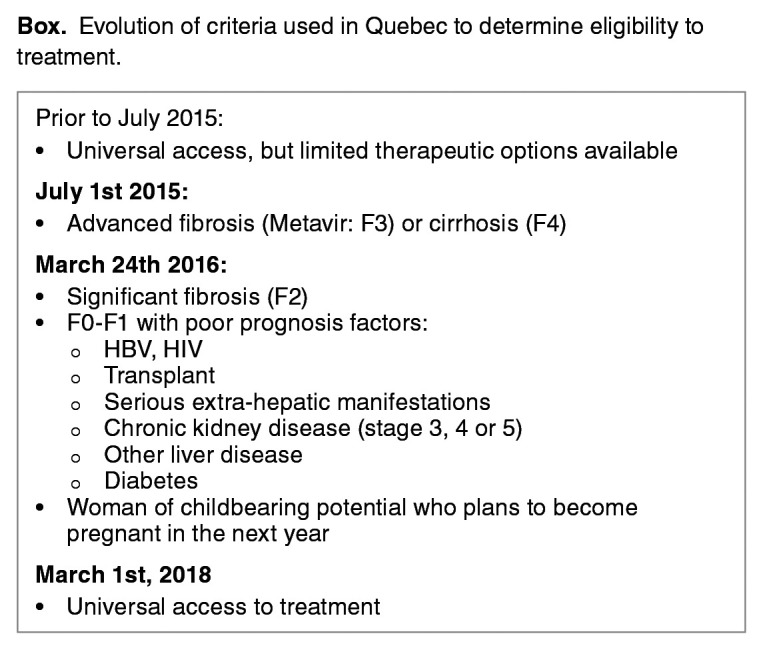
背景:从历史上看,丙型肝炎病毒(HCV)预处理评估需要多次访问,经常导致失去随访和延迟开始治疗。新技术可以加速这一进程。我们调查了一天评估计划的可行性及其对注射吸毒者(PWIDs)评估完成情况、治疗资格意识和治疗启动的影响。方法:招募不知道自己是否有资格接受治疗的hcv感染PWID,在2017年至2019年期间对加速治疗模式进行前瞻性评估,并与历史队列进行比较。患者在一次访问中接受了医学评估、快速HCV病毒载量检测和短暂弹性成像,最后告知他们是否有资格接受治疗。2014年至2016年期间在成瘾医学诊所接受检查的患者,符合相同的纳入标准,并以通常的护理标准进行评估,作为对照组。结果:加速队列和历史队列分别包括99例和76例患者。这些队列在年龄和性别上没有显著差异,但历史队列中更多的患者正在接受阿片类激动剂治疗,而加速队列中更多的患者在上个月注射了药物。加速评估导致更高的评估完成率(100% vs 67.1%;p = .28)。加速队列中开始治疗的延迟时间比历史队列短(69 (IQR: 49-106)天和219 (IQR: 141-416)天;结论:加速评估提高了合格患者的资格意识,缩短了开始治疗的时间。试验注册:本研究在www.clinicaltrials.gov (NCT02755402)上注册。
Impact of an Accelerated Pretreatment Evaluation on Linkage-to-Care for Hepatitis C-infected Persons Who Inject Drugs.
Background: Historically, hepatitis C virus (HCV) pretreatment evaluation has required multiple visits, frequently resulting in loss to follow-up and a delayed initiation of treatment. New technologies can accelerate this process. We investigated the feasibility of a single-day evaluation program and its impact on evaluation completion, treatment eligibility awareness, and treatment initiation among people who inject drugs (PWIDs).
Methods: HCV-infected PWID who were unaware if they were eligible for treatment were recruited in a prospective evaluation of an accelerated model of care between 2017 and 2019 and compared to a historical cohort. The patients underwent a medical evaluation, rapid HCV viral load testing, and transient elastography during a single visit, at the end of which they were informed whether they were eligible for treatment. A historical cohort of patients fulfilling the same inclusion criteria and evaluated with the usual standard of care spanning several visits who were examined at the addiction medicine clinic from 2014 to 2016 served as the comparison group.
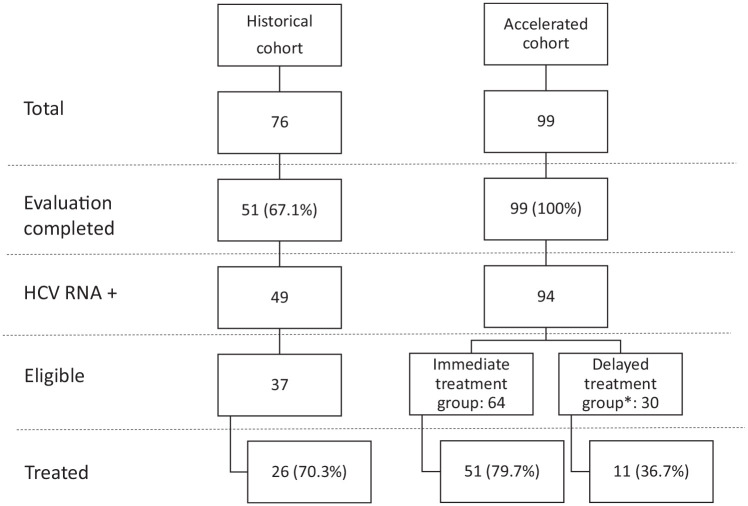
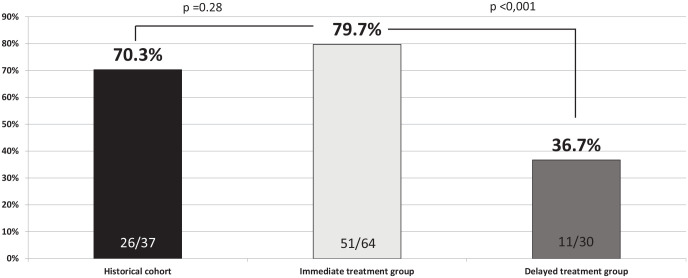
Results: The accelerated and historical cohorts included 99 and 76 patients, respectively. The cohorts did not differ significantly by age and gender, but more patients in the historical cohort were undergoing opioid agonist therapy, while more patients in the accelerated cohort injected drugs in the last month. An accelerated evaluation resulted in a higher rate of evaluation completion (100% vs 67.1%; P < .001). Among those eligible for treatment, the proportion of those initiating treatment was similar between the groups (51/64 (79.7%) vs. 26/37 (70.3%); P = .28). The delay in the initiation of treatment was shorter in the accelerated cohort than in the historical cohort (69 (IQR: 49-106) days vs. 219 (IQR: 141-416) days; P < .001).
Conclusions: Accelerated evaluation enhanced the awareness of eligibility and reduced the time to initiation among eligible patients.
Trial registration: This study is registered on www.clinicaltrials.gov (NCT02755402).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


