Melissa L Arvay, Nong Shang, Shamim A Qazi, Gary L Darmstadt, Mohammad Shahidul Islam, Daniel E Roth, Anran Liu, Nicholas E Connor, Belal Hossain, Qazi Sadeq-Ur Rahman, Shams El Arifeen, Luke C Mullany, Anita K M Zaidi, Zulfiqar A Bhutta, Sajid B Soofi, Yasir Shafiq, Abdullah H Baqui, Dipak K Mitra, Pinaki Panigrahi, Kalpana Panigrahi, Anuradha Bose, Rita Isaac, Daniel Westreich, Steven R Meshnick, Samir K Saha, Stephanie J Schrag
{"title":"使用世卫组织定义分类的南亚新生儿疾病的感染病因:对ANISA研究的初步分析。","authors":"Melissa L Arvay, Nong Shang, Shamim A Qazi, Gary L Darmstadt, Mohammad Shahidul Islam, Daniel E Roth, Anran Liu, Nicholas E Connor, Belal Hossain, Qazi Sadeq-Ur Rahman, Shams El Arifeen, Luke C Mullany, Anita K M Zaidi, Zulfiqar A Bhutta, Sajid B Soofi, Yasir Shafiq, Abdullah H Baqui, Dipak K Mitra, Pinaki Panigrahi, Kalpana Panigrahi, Anuradha Bose, Rita Isaac, Daniel Westreich, Steven R Meshnick, Samir K Saha, Stephanie J Schrag","doi":"10.1016/S2214-109X(22)00244-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Globally, neonatal mortality accounts for almost half of all deaths in children younger than 5 years. Aetiological agents of neonatal infection are difficult to identify because the clinical signs are non-specific. Using data from the Aetiology of Neonatal Infections in south Asia (ANISA) cohort, we aimed to describe the spectrum of infectious aetiologies of acute neonatal illness categorised post-hoc using the 2015 WHO case definitions of critical illness, clinical severe infection, and fast breathing only.</p><p><strong>Methods: </strong>Eligible infants were aged 0-59 days with possible serious bacterial infection and healthy infants enrolled in the ANISA study in Bangladesh, India, and Pakistan. We applied a partial latent class Bayesian model to estimate the prevalence of 27 pathogens detectable on PCR, pathogens detected by blood culture only, and illness not attributed to any infectious aetiology. Infants with at least one clinical specimen available were included in the analysis. We assessed the prevalence of these aetiologies according to WHO's case definitions of critically ill, clinical severe infection, and infants with late onset, isolated fast breathing. For the clinical severe definition, we compared the prevalence of signs by bacterial versus viral aetiology.</p><p><strong>Findings: </strong>There were 934 infants (992 episodes) in the critically ill category, 3769 (4000 episodes) in the clinical severe infection category, and 738 (771 episodes) in the late-onset isolated fast breathing category. We estimated the proportion of illness attributable to bacterial infection was 32·7% in infants in the critically ill group, 15·6% in the clinical severe infection group, and 8·8% among infants with late-onset isolated fast breathing group. An infectious aetiology was not identified in 58-82% of infants in these categories. Among 4000 episodes of clinical severe infection, those with bacterial versus viral attribution had higher proportions of hypothermia, movement only when stimulated, convulsions, and poor feeding.</p><p><strong>Interpretation: </strong>Our modelled results generally support the revised WHO case definitions, although a revision of the most severe case definition could be considered. Clinical criteria do not clearly differentiate between young infants with and without infectious aetiologies. Our results highlight the need for improved point-of-care diagnostics, and further study into neonatal deaths and episodes with no identified aetiology, to ensure antibiotic stewardship and targeted interventions.</p><p><strong>Funding: </strong>The Bill and Melinda Gates Foundation.</p>","PeriodicalId":153380,"journal":{"name":"The Lancet. Global health","volume":" ","pages":"e1289-e1297"},"PeriodicalIF":0.0000,"publicationDate":"2022-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9380253/pdf/","citationCount":"0","resultStr":"{\"title\":\"Infectious aetiologies of neonatal illness in south Asia classified using WHO definitions: a primary analysis of the ANISA study.\",\"authors\":\"Melissa L Arvay, Nong Shang, Shamim A Qazi, Gary L Darmstadt, Mohammad Shahidul Islam, Daniel E Roth, Anran Liu, Nicholas E Connor, Belal Hossain, Qazi Sadeq-Ur Rahman, Shams El Arifeen, Luke C Mullany, Anita K M Zaidi, Zulfiqar A Bhutta, Sajid B Soofi, Yasir Shafiq, Abdullah H Baqui, Dipak K Mitra, Pinaki Panigrahi, Kalpana Panigrahi, Anuradha Bose, Rita Isaac, Daniel Westreich, Steven R Meshnick, Samir K Saha, Stephanie J Schrag\",\"doi\":\"10.1016/S2214-109X(22)00244-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Globally, neonatal mortality accounts for almost half of all deaths in children younger than 5 years. Aetiological agents of neonatal infection are difficult to identify because the clinical signs are non-specific. Using data from the Aetiology of Neonatal Infections in south Asia (ANISA) cohort, we aimed to describe the spectrum of infectious aetiologies of acute neonatal illness categorised post-hoc using the 2015 WHO case definitions of critical illness, clinical severe infection, and fast breathing only.</p><p><strong>Methods: </strong>Eligible infants were aged 0-59 days with possible serious bacterial infection and healthy infants enrolled in the ANISA study in Bangladesh, India, and Pakistan. We applied a partial latent class Bayesian model to estimate the prevalence of 27 pathogens detectable on PCR, pathogens detected by blood culture only, and illness not attributed to any infectious aetiology. Infants with at least one clinical specimen available were included in the analysis. We assessed the prevalence of these aetiologies according to WHO's case definitions of critically ill, clinical severe infection, and infants with late onset, isolated fast breathing. For the clinical severe definition, we compared the prevalence of signs by bacterial versus viral aetiology.</p><p><strong>Findings: </strong>There were 934 infants (992 episodes) in the critically ill category, 3769 (4000 episodes) in the clinical severe infection category, and 738 (771 episodes) in the late-onset isolated fast breathing category. We estimated the proportion of illness attributable to bacterial infection was 32·7% in infants in the critically ill group, 15·6% in the clinical severe infection group, and 8·8% among infants with late-onset isolated fast breathing group. An infectious aetiology was not identified in 58-82% of infants in these categories. Among 4000 episodes of clinical severe infection, those with bacterial versus viral attribution had higher proportions of hypothermia, movement only when stimulated, convulsions, and poor feeding.</p><p><strong>Interpretation: </strong>Our modelled results generally support the revised WHO case definitions, although a revision of the most severe case definition could be considered. Clinical criteria do not clearly differentiate between young infants with and without infectious aetiologies. Our results highlight the need for improved point-of-care diagnostics, and further study into neonatal deaths and episodes with no identified aetiology, to ensure antibiotic stewardship and targeted interventions.</p><p><strong>Funding: </strong>The Bill and Melinda Gates Foundation.</p>\",\"PeriodicalId\":153380,\"journal\":{\"name\":\"The Lancet. Global health\",\"volume\":\" \",\"pages\":\"e1289-e1297\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9380253/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Lancet. Global health\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1016/S2214-109X(22)00244-3\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Lancet. Global health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1016/S2214-109X(22)00244-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Infectious aetiologies of neonatal illness in south Asia classified using WHO definitions: a primary analysis of the ANISA study.
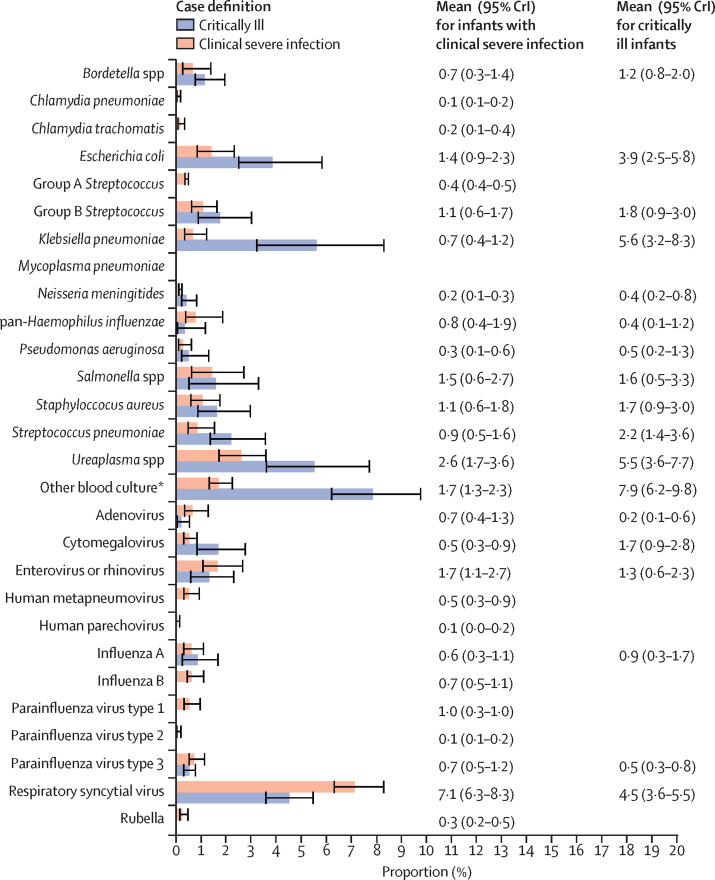
Background: Globally, neonatal mortality accounts for almost half of all deaths in children younger than 5 years. Aetiological agents of neonatal infection are difficult to identify because the clinical signs are non-specific. Using data from the Aetiology of Neonatal Infections in south Asia (ANISA) cohort, we aimed to describe the spectrum of infectious aetiologies of acute neonatal illness categorised post-hoc using the 2015 WHO case definitions of critical illness, clinical severe infection, and fast breathing only.
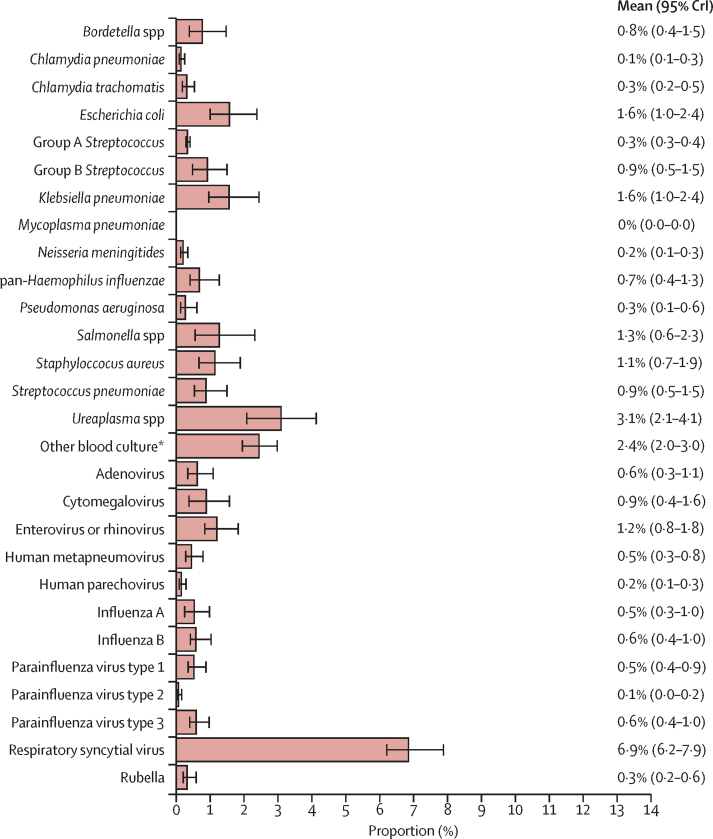
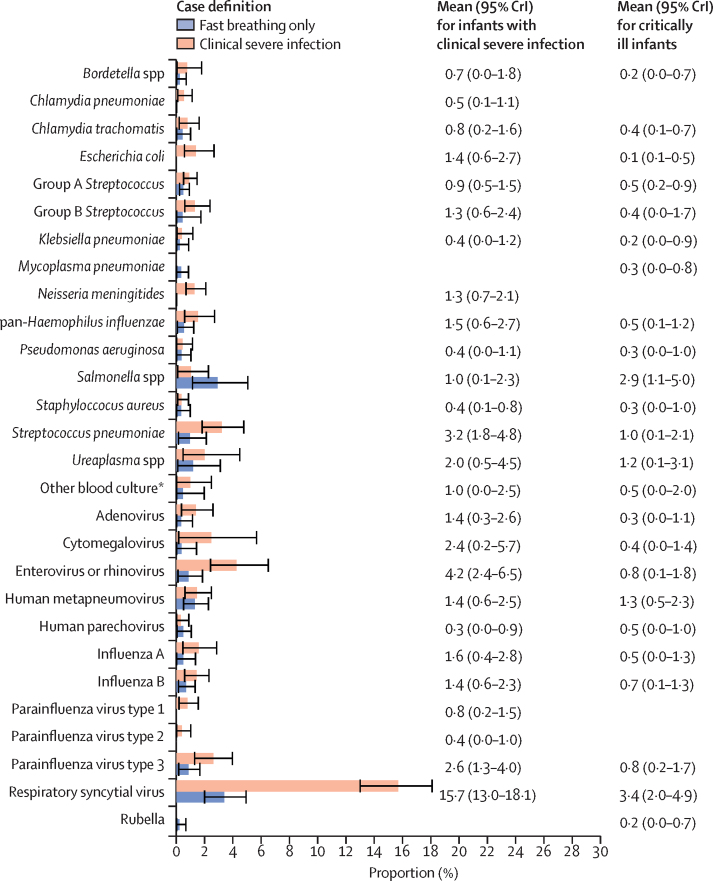
Methods: Eligible infants were aged 0-59 days with possible serious bacterial infection and healthy infants enrolled in the ANISA study in Bangladesh, India, and Pakistan. We applied a partial latent class Bayesian model to estimate the prevalence of 27 pathogens detectable on PCR, pathogens detected by blood culture only, and illness not attributed to any infectious aetiology. Infants with at least one clinical specimen available were included in the analysis. We assessed the prevalence of these aetiologies according to WHO's case definitions of critically ill, clinical severe infection, and infants with late onset, isolated fast breathing. For the clinical severe definition, we compared the prevalence of signs by bacterial versus viral aetiology.
Findings: There were 934 infants (992 episodes) in the critically ill category, 3769 (4000 episodes) in the clinical severe infection category, and 738 (771 episodes) in the late-onset isolated fast breathing category. We estimated the proportion of illness attributable to bacterial infection was 32·7% in infants in the critically ill group, 15·6% in the clinical severe infection group, and 8·8% among infants with late-onset isolated fast breathing group. An infectious aetiology was not identified in 58-82% of infants in these categories. Among 4000 episodes of clinical severe infection, those with bacterial versus viral attribution had higher proportions of hypothermia, movement only when stimulated, convulsions, and poor feeding.
Interpretation: Our modelled results generally support the revised WHO case definitions, although a revision of the most severe case definition could be considered. Clinical criteria do not clearly differentiate between young infants with and without infectious aetiologies. Our results highlight the need for improved point-of-care diagnostics, and further study into neonatal deaths and episodes with no identified aetiology, to ensure antibiotic stewardship and targeted interventions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


