Andrea Katharina Lindner, Anna Katharina Luger, Josef Fritz, Johannes Stäblein, Christian Radmayr, Friedrich Aigner, Peter Rehder, Gennadi Tulchiner, Wolfgang Horninger, Renate Pichler
{"title":"单纯钝性肾损伤是否需要重复CT扫描?大容量泌尿创伤中心的经验。","authors":"Andrea Katharina Lindner, Anna Katharina Luger, Josef Fritz, Johannes Stäblein, Christian Radmayr, Friedrich Aigner, Peter Rehder, Gennadi Tulchiner, Wolfgang Horninger, Renate Pichler","doi":"10.1186/s13017-022-00445-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Current guidelines recommend repeat computed tomography (CT) imaging in high-grade blunt renal injury within 48-96 h, yet diagnostic value and clinical significance remain controversial. The aim of this work was to determine the possible gain of CT re-imaging in uncomplicated patients with blunt renal trauma at 48 h after injury, presenting one of the largest case series.</p><p><strong>Methods: </strong>A retrospective database of patients admitted to our centre with isolated blunt renal trauma due to sporting injuries was analysed for a period of 20 years (2000-2020). We included only patients who underwent repeat imaging at 48 h after trauma irrespective of AAST renal injury grading (grade 1-5) and initial management. The primary outcome was intervention rates after CT imaging at 48 h in uncomplicated patients versus CT scan at the time of clinical symptoms.</p><p><strong>Results: </strong>A total of 280 patients (mean age: 37.8 years; 244 (87.1%) male) with repeat CT after 48 h were included. 150 (53.6%) patients were classified as low-grade (grade 1-3) and 130 (46.4%) as high-grade (grade 4-5) trauma. Immediate intervention at trauma was necessary in 59 (21.1%) patients with high-grade injuries: minimally invasive therapy in 48 (81.4%) and open surgery in 11 (18.6%) patients, respectively. In only 16 (5.7%) cases, intervention was performed based on CT re-imaging at 48 h (low-grade vs. high-grade: 3.3% vs. 8.5%; p = 0.075). On the contrary, intervention rate due to clinical symptoms was 12.5% (n = 35). Onset of clinical progress was on average (range) 5.3 (1-17) days post trauma. High-grade trauma (odds ratio [OR]<sub>grade 4 vs. grade 3</sub>, 14.62; p < 0.001; OR<sub>grade 5 vs. grade 3</sub>, 22.88, p = 0.004) and intervention performed at the day of trauma (OR 3.22; p = 0.014) were powerful predictors of occurrence of clinical progress.</p><p><strong>Conclusion: </strong>Our data suggest that routine CT imaging 48 h post trauma can be safely omitted for patients with low- and high-grade blunt renal injury as long as they remain clinically stable. Patients with high-grade renal injury have the highest risk for clinical progress; thus, close surveillance should be considered especially in this group.</p>","PeriodicalId":290899,"journal":{"name":"World Journal of Emergency Surgery : WJES","volume":" ","pages":"38"},"PeriodicalIF":0.0000,"publicationDate":"2022-07-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9264658/pdf/","citationCount":"1","resultStr":"{\"title\":\"Do we need repeated CT imaging in uncomplicated blunt renal injuries? Experiences of a high-volume urological trauma centre.\",\"authors\":\"Andrea Katharina Lindner, Anna Katharina Luger, Josef Fritz, Johannes Stäblein, Christian Radmayr, Friedrich Aigner, Peter Rehder, Gennadi Tulchiner, Wolfgang Horninger, Renate Pichler\",\"doi\":\"10.1186/s13017-022-00445-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Current guidelines recommend repeat computed tomography (CT) imaging in high-grade blunt renal injury within 48-96 h, yet diagnostic value and clinical significance remain controversial. The aim of this work was to determine the possible gain of CT re-imaging in uncomplicated patients with blunt renal trauma at 48 h after injury, presenting one of the largest case series.</p><p><strong>Methods: </strong>A retrospective database of patients admitted to our centre with isolated blunt renal trauma due to sporting injuries was analysed for a period of 20 years (2000-2020). We included only patients who underwent repeat imaging at 48 h after trauma irrespective of AAST renal injury grading (grade 1-5) and initial management. The primary outcome was intervention rates after CT imaging at 48 h in uncomplicated patients versus CT scan at the time of clinical symptoms.</p><p><strong>Results: </strong>A total of 280 patients (mean age: 37.8 years; 244 (87.1%) male) with repeat CT after 48 h were included. 150 (53.6%) patients were classified as low-grade (grade 1-3) and 130 (46.4%) as high-grade (grade 4-5) trauma. Immediate intervention at trauma was necessary in 59 (21.1%) patients with high-grade injuries: minimally invasive therapy in 48 (81.4%) and open surgery in 11 (18.6%) patients, respectively. In only 16 (5.7%) cases, intervention was performed based on CT re-imaging at 48 h (low-grade vs. high-grade: 3.3% vs. 8.5%; p = 0.075). On the contrary, intervention rate due to clinical symptoms was 12.5% (n = 35). Onset of clinical progress was on average (range) 5.3 (1-17) days post trauma. High-grade trauma (odds ratio [OR]<sub>grade 4 vs. grade 3</sub>, 14.62; p < 0.001; OR<sub>grade 5 vs. grade 3</sub>, 22.88, p = 0.004) and intervention performed at the day of trauma (OR 3.22; p = 0.014) were powerful predictors of occurrence of clinical progress.</p><p><strong>Conclusion: </strong>Our data suggest that routine CT imaging 48 h post trauma can be safely omitted for patients with low- and high-grade blunt renal injury as long as they remain clinically stable. Patients with high-grade renal injury have the highest risk for clinical progress; thus, close surveillance should be considered especially in this group.</p>\",\"PeriodicalId\":290899,\"journal\":{\"name\":\"World Journal of Emergency Surgery : WJES\",\"volume\":\" \",\"pages\":\"38\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-07-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9264658/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Emergency Surgery : WJES\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13017-022-00445-9\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Emergency Surgery : WJES","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13017-022-00445-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Do we need repeated CT imaging in uncomplicated blunt renal injuries? Experiences of a high-volume urological trauma centre.
Background: Current guidelines recommend repeat computed tomography (CT) imaging in high-grade blunt renal injury within 48-96 h, yet diagnostic value and clinical significance remain controversial. The aim of this work was to determine the possible gain of CT re-imaging in uncomplicated patients with blunt renal trauma at 48 h after injury, presenting one of the largest case series.
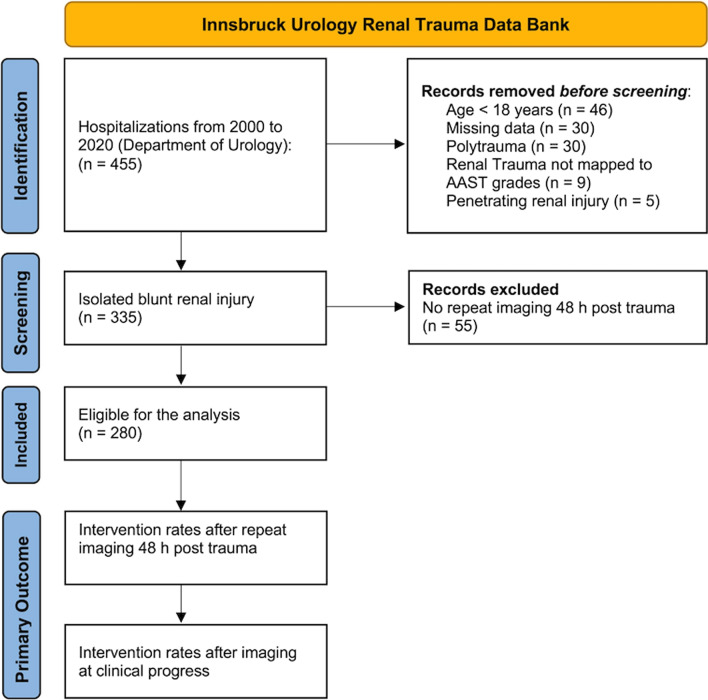
Methods: A retrospective database of patients admitted to our centre with isolated blunt renal trauma due to sporting injuries was analysed for a period of 20 years (2000-2020). We included only patients who underwent repeat imaging at 48 h after trauma irrespective of AAST renal injury grading (grade 1-5) and initial management. The primary outcome was intervention rates after CT imaging at 48 h in uncomplicated patients versus CT scan at the time of clinical symptoms.
Results: A total of 280 patients (mean age: 37.8 years; 244 (87.1%) male) with repeat CT after 48 h were included. 150 (53.6%) patients were classified as low-grade (grade 1-3) and 130 (46.4%) as high-grade (grade 4-5) trauma. Immediate intervention at trauma was necessary in 59 (21.1%) patients with high-grade injuries: minimally invasive therapy in 48 (81.4%) and open surgery in 11 (18.6%) patients, respectively. In only 16 (5.7%) cases, intervention was performed based on CT re-imaging at 48 h (low-grade vs. high-grade: 3.3% vs. 8.5%; p = 0.075). On the contrary, intervention rate due to clinical symptoms was 12.5% (n = 35). Onset of clinical progress was on average (range) 5.3 (1-17) days post trauma. High-grade trauma (odds ratio [OR]grade 4 vs. grade 3, 14.62; p < 0.001; ORgrade 5 vs. grade 3, 22.88, p = 0.004) and intervention performed at the day of trauma (OR 3.22; p = 0.014) were powerful predictors of occurrence of clinical progress.
Conclusion: Our data suggest that routine CT imaging 48 h post trauma can be safely omitted for patients with low- and high-grade blunt renal injury as long as they remain clinically stable. Patients with high-grade renal injury have the highest risk for clinical progress; thus, close surveillance should be considered especially in this group.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


