{"title":"职业性超敏性肺炎暴露于聚氨酯胶粘剂后。","authors":"Arbaaz Patel, Aasim Hasany, Susan M Tarlo","doi":"10.1503/cmaj.220052","DOIUrl":null,"url":null,"abstract":"CMAJ | August 2, 2022 | Volume 194 | Issue 29 E1027 A 47-year-old woman presented to hospital with a 3-month history of dry cough, wheeze, dyspnea and intermittent fever. She had been briefly admitted 2 months earlier to treat a presumed lower respiratory tract infection or bronchitis; she had been prescribed inhalers (salbutamol, ipratropium) and antibiotics (ceftriaxone and azithromycin initially and then amoxicillin–clavulanic acid). The patient had smoked 7 cigarettes per day for 12 years, but had stopped smoking 3 months earlier. She was not on any regular medications and her medical history was notable only for obstructive sleep apnea, which was treated with continuous positive airway pressure. She had no history of asthma, no pets and no exposures to hot tubs, birds or moulds at home. She had recently started working at a horticultural company where she made plug sets for plants, in which soil, adhesives, oil and water were combined to create stable moulds for seedlings. The patient’s chest radiograph was normal on presentation and unchanged from her previous admission 2 months earlier. She was referred to the inpatient respirology service. When assessed, her respiratory rate was 22 breaths/min, oxygen saturation was 96% on room air, temperature was 35.9°C, heart rate was 104 beats/min and blood pressure was 129/86 mm Hg. She had wheezes bilaterally and normal heart sounds. On examination, she had no evidence of finger clubbing, leg edema, rashes or features to suggest a connective tissue disorder. The emergency department physician ordered a computed tomography (CT) scan of the chest with contrast (pulmonary embolus protocol) to rule out pulmonary embolism. Figure 1 is a representative chest CT image from the time of hospital admission, showing diffuse centrilobular ground glass nodules in both lungs without any zonal predominance. There were no pulmonary emboli. The patient had substantial leukocytosis with neutrophilia (leukocytes 15.6 [normal 4.0–11.0] × 109/L, neutrophils 12.0 [normal 2.0–7.5] × 109/L), a normal eosinophil count (0.2 [normal 0.0–0.5] × 109/L) and an elevated C-reactive protein (49 [normal < 8 mg/L). Because interstitial lung disease was suspected, rheumatoid factor, antinuclear antibody, and cytoplasmic and perinuclear antineutrophil cytoplasmic antibody levels were ordered and were all negative. Brain natriuretic peptide and troponin levels, ordered by an emergency department physician, were within normal limits on both visits to hospital. Spirometry showed proportionate reduction in forced expiratory volume at 1 second (FEV1) and forced vital capacity (FVC), with no evidence of obstruction. Her FVC was 2.13 L (59% predicted), her FEV1 was 1.54 L (53% predicted) and her FEV1:FVC ratio was 72.3%. A bronchoscopy with bronchoalveolar lavage and transbronchial biopsy was performed. The fluid from bronchoalveolar Practice | Cases CPD","PeriodicalId":520595,"journal":{"name":"CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne","volume":" ","pages":"E1027-E1030"},"PeriodicalIF":0.0000,"publicationDate":"2022-08-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/cf/ec/194e1027.PMC9481262.pdf","citationCount":"2","resultStr":"{\"title\":\"Occupational hypersensitivity pneumonitis after polyurethane adhesive exposure.\",\"authors\":\"Arbaaz Patel, Aasim Hasany, Susan M Tarlo\",\"doi\":\"10.1503/cmaj.220052\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"CMAJ | August 2, 2022 | Volume 194 | Issue 29 E1027 A 47-year-old woman presented to hospital with a 3-month history of dry cough, wheeze, dyspnea and intermittent fever. She had been briefly admitted 2 months earlier to treat a presumed lower respiratory tract infection or bronchitis; she had been prescribed inhalers (salbutamol, ipratropium) and antibiotics (ceftriaxone and azithromycin initially and then amoxicillin–clavulanic acid). The patient had smoked 7 cigarettes per day for 12 years, but had stopped smoking 3 months earlier. She was not on any regular medications and her medical history was notable only for obstructive sleep apnea, which was treated with continuous positive airway pressure. She had no history of asthma, no pets and no exposures to hot tubs, birds or moulds at home. She had recently started working at a horticultural company where she made plug sets for plants, in which soil, adhesives, oil and water were combined to create stable moulds for seedlings. The patient’s chest radiograph was normal on presentation and unchanged from her previous admission 2 months earlier. She was referred to the inpatient respirology service. When assessed, her respiratory rate was 22 breaths/min, oxygen saturation was 96% on room air, temperature was 35.9°C, heart rate was 104 beats/min and blood pressure was 129/86 mm Hg. She had wheezes bilaterally and normal heart sounds. On examination, she had no evidence of finger clubbing, leg edema, rashes or features to suggest a connective tissue disorder. The emergency department physician ordered a computed tomography (CT) scan of the chest with contrast (pulmonary embolus protocol) to rule out pulmonary embolism. Figure 1 is a representative chest CT image from the time of hospital admission, showing diffuse centrilobular ground glass nodules in both lungs without any zonal predominance. There were no pulmonary emboli. The patient had substantial leukocytosis with neutrophilia (leukocytes 15.6 [normal 4.0–11.0] × 109/L, neutrophils 12.0 [normal 2.0–7.5] × 109/L), a normal eosinophil count (0.2 [normal 0.0–0.5] × 109/L) and an elevated C-reactive protein (49 [normal < 8 mg/L). Because interstitial lung disease was suspected, rheumatoid factor, antinuclear antibody, and cytoplasmic and perinuclear antineutrophil cytoplasmic antibody levels were ordered and were all negative. Brain natriuretic peptide and troponin levels, ordered by an emergency department physician, were within normal limits on both visits to hospital. Spirometry showed proportionate reduction in forced expiratory volume at 1 second (FEV1) and forced vital capacity (FVC), with no evidence of obstruction. Her FVC was 2.13 L (59% predicted), her FEV1 was 1.54 L (53% predicted) and her FEV1:FVC ratio was 72.3%. A bronchoscopy with bronchoalveolar lavage and transbronchial biopsy was performed. The fluid from bronchoalveolar Practice | Cases CPD\",\"PeriodicalId\":520595,\"journal\":{\"name\":\"CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne\",\"volume\":\" \",\"pages\":\"E1027-E1030\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-08-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/cf/ec/194e1027.PMC9481262.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1503/cmaj.220052\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1503/cmaj.220052","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Occupational hypersensitivity pneumonitis after polyurethane adhesive exposure.
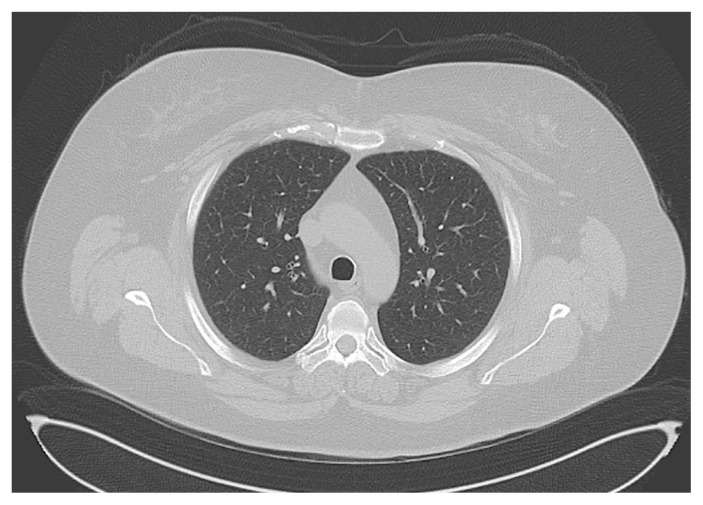
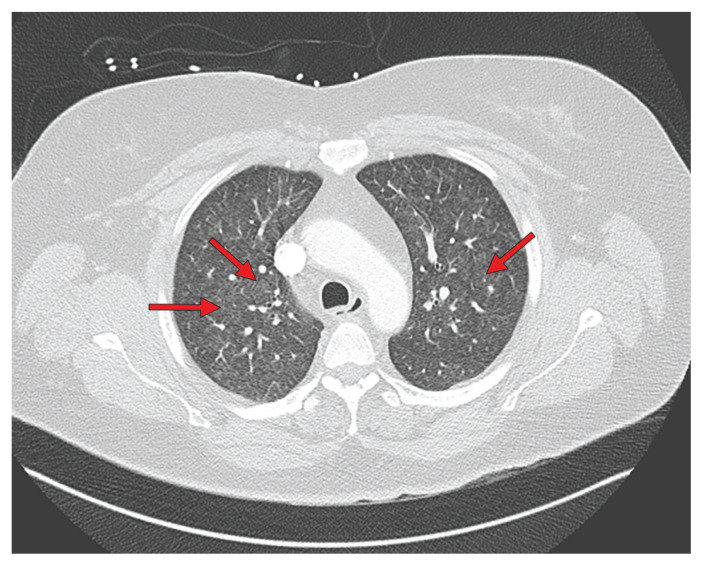
CMAJ | August 2, 2022 | Volume 194 | Issue 29 E1027 A 47-year-old woman presented to hospital with a 3-month history of dry cough, wheeze, dyspnea and intermittent fever. She had been briefly admitted 2 months earlier to treat a presumed lower respiratory tract infection or bronchitis; she had been prescribed inhalers (salbutamol, ipratropium) and antibiotics (ceftriaxone and azithromycin initially and then amoxicillin–clavulanic acid). The patient had smoked 7 cigarettes per day for 12 years, but had stopped smoking 3 months earlier. She was not on any regular medications and her medical history was notable only for obstructive sleep apnea, which was treated with continuous positive airway pressure. She had no history of asthma, no pets and no exposures to hot tubs, birds or moulds at home. She had recently started working at a horticultural company where she made plug sets for plants, in which soil, adhesives, oil and water were combined to create stable moulds for seedlings. The patient’s chest radiograph was normal on presentation and unchanged from her previous admission 2 months earlier. She was referred to the inpatient respirology service. When assessed, her respiratory rate was 22 breaths/min, oxygen saturation was 96% on room air, temperature was 35.9°C, heart rate was 104 beats/min and blood pressure was 129/86 mm Hg. She had wheezes bilaterally and normal heart sounds. On examination, she had no evidence of finger clubbing, leg edema, rashes or features to suggest a connective tissue disorder. The emergency department physician ordered a computed tomography (CT) scan of the chest with contrast (pulmonary embolus protocol) to rule out pulmonary embolism. Figure 1 is a representative chest CT image from the time of hospital admission, showing diffuse centrilobular ground glass nodules in both lungs without any zonal predominance. There were no pulmonary emboli. The patient had substantial leukocytosis with neutrophilia (leukocytes 15.6 [normal 4.0–11.0] × 109/L, neutrophils 12.0 [normal 2.0–7.5] × 109/L), a normal eosinophil count (0.2 [normal 0.0–0.5] × 109/L) and an elevated C-reactive protein (49 [normal < 8 mg/L). Because interstitial lung disease was suspected, rheumatoid factor, antinuclear antibody, and cytoplasmic and perinuclear antineutrophil cytoplasmic antibody levels were ordered and were all negative. Brain natriuretic peptide and troponin levels, ordered by an emergency department physician, were within normal limits on both visits to hospital. Spirometry showed proportionate reduction in forced expiratory volume at 1 second (FEV1) and forced vital capacity (FVC), with no evidence of obstruction. Her FVC was 2.13 L (59% predicted), her FEV1 was 1.54 L (53% predicted) and her FEV1:FVC ratio was 72.3%. A bronchoscopy with bronchoalveolar lavage and transbronchial biopsy was performed. The fluid from bronchoalveolar Practice | Cases CPD

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


