Albert Youngwoo Jang, Su Jung Park, Wook-Jin Chung
{"title":"心力衰竭患者的肺动脉高压。","authors":"Albert Youngwoo Jang, Su Jung Park, Wook-Jin Chung","doi":"10.36628/ijhf.2020.0053","DOIUrl":null,"url":null,"abstract":"<p><p>Pulmonary hypertension (PH) is traditionally defined as a mean pulmonary arterial pressure (mPAP) ≥25 mmHg. Although various factors cause PH, the most common etiology is PH due to left heart disease (PH-LHD). The underlying LHD is characterized by heart failure (HF) with reduced ejection fraction (HFrEF), HF with preserved ejection fraction (HFpEF), valvular heart disease, cardiomyopathies, or arrhythmic diseases. Regardless of its underlying cause, elevated left atrial (LA) filling pressure is a manifestation of advanced heart disease. High LA pressure then causes persistent backflow to the pulmonary veins, which increases mPAP. PH-LHD at this stage is named isolated postcapillary PH (IpcPH). Further progression of IpcPH is associated with pulmonary vasculature remodeling and hypertrophy, which consists of adding the precapillary component of PH to the pre-existing postcapillary PH. This form of PH-LHD is called combined precapillary and postcapillary PH (CpcPH). To date, therapeutic strategies for PH-LHD have been investigated in the context of HFrEF or HFpEF. Pulmonary arterial hypertension (PAH)-specific drugs have been tested in HFrEF and HFpEF populations, although encouraging results have not been demonstrated. As PAH-specific drugs target the precapillary component of PH-LHD, future studies utilizing such therapeutics in PH-LHD patients with CpcPH appear to have a more robust pathobiological basis. This article reviews the diagnosis, pathophysiology, treatment, and future direction of PH in HF.</p>","PeriodicalId":14058,"journal":{"name":"International Journal of Heart Failure","volume":"3 3","pages":"147-159"},"PeriodicalIF":0.0000,"publicationDate":"2021-04-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1b/18/ijhf-3-147.PMC9536651.pdf","citationCount":"0","resultStr":"{\"title\":\"Pulmonary Hypertension in Heart Failure.\",\"authors\":\"Albert Youngwoo Jang, Su Jung Park, Wook-Jin Chung\",\"doi\":\"10.36628/ijhf.2020.0053\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Pulmonary hypertension (PH) is traditionally defined as a mean pulmonary arterial pressure (mPAP) ≥25 mmHg. Although various factors cause PH, the most common etiology is PH due to left heart disease (PH-LHD). The underlying LHD is characterized by heart failure (HF) with reduced ejection fraction (HFrEF), HF with preserved ejection fraction (HFpEF), valvular heart disease, cardiomyopathies, or arrhythmic diseases. Regardless of its underlying cause, elevated left atrial (LA) filling pressure is a manifestation of advanced heart disease. High LA pressure then causes persistent backflow to the pulmonary veins, which increases mPAP. PH-LHD at this stage is named isolated postcapillary PH (IpcPH). Further progression of IpcPH is associated with pulmonary vasculature remodeling and hypertrophy, which consists of adding the precapillary component of PH to the pre-existing postcapillary PH. This form of PH-LHD is called combined precapillary and postcapillary PH (CpcPH). To date, therapeutic strategies for PH-LHD have been investigated in the context of HFrEF or HFpEF. Pulmonary arterial hypertension (PAH)-specific drugs have been tested in HFrEF and HFpEF populations, although encouraging results have not been demonstrated. As PAH-specific drugs target the precapillary component of PH-LHD, future studies utilizing such therapeutics in PH-LHD patients with CpcPH appear to have a more robust pathobiological basis. This article reviews the diagnosis, pathophysiology, treatment, and future direction of PH in HF.</p>\",\"PeriodicalId\":14058,\"journal\":{\"name\":\"International Journal of Heart Failure\",\"volume\":\"3 3\",\"pages\":\"147-159\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-04-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1b/18/ijhf-3-147.PMC9536651.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Heart Failure\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.36628/ijhf.2020.0053\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Heart Failure","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36628/ijhf.2020.0053","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
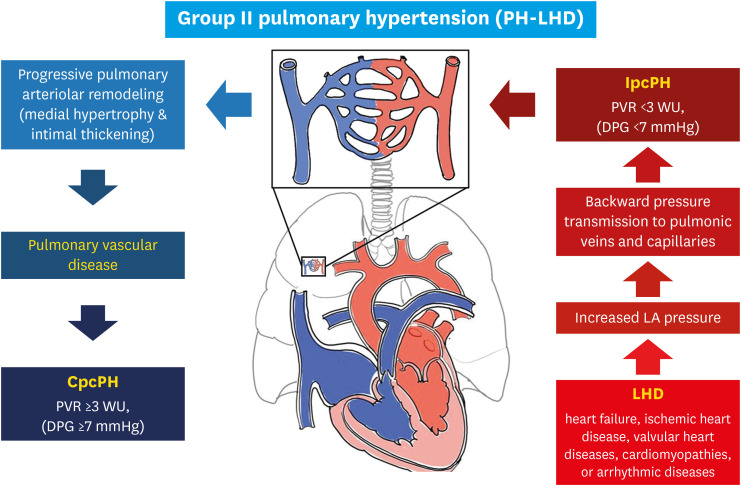
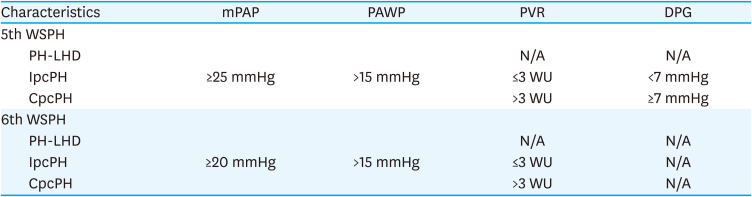
Pulmonary hypertension (PH) is traditionally defined as a mean pulmonary arterial pressure (mPAP) ≥25 mmHg. Although various factors cause PH, the most common etiology is PH due to left heart disease (PH-LHD). The underlying LHD is characterized by heart failure (HF) with reduced ejection fraction (HFrEF), HF with preserved ejection fraction (HFpEF), valvular heart disease, cardiomyopathies, or arrhythmic diseases. Regardless of its underlying cause, elevated left atrial (LA) filling pressure is a manifestation of advanced heart disease. High LA pressure then causes persistent backflow to the pulmonary veins, which increases mPAP. PH-LHD at this stage is named isolated postcapillary PH (IpcPH). Further progression of IpcPH is associated with pulmonary vasculature remodeling and hypertrophy, which consists of adding the precapillary component of PH to the pre-existing postcapillary PH. This form of PH-LHD is called combined precapillary and postcapillary PH (CpcPH). To date, therapeutic strategies for PH-LHD have been investigated in the context of HFrEF or HFpEF. Pulmonary arterial hypertension (PAH)-specific drugs have been tested in HFrEF and HFpEF populations, although encouraging results have not been demonstrated. As PAH-specific drugs target the precapillary component of PH-LHD, future studies utilizing such therapeutics in PH-LHD patients with CpcPH appear to have a more robust pathobiological basis. This article reviews the diagnosis, pathophysiology, treatment, and future direction of PH in HF.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


