{"title":"南非儿科重症监护室对创伤后癫痫发作的药物治疗。","authors":"N Yachad, K D Naidoo","doi":"10.7196/SAJCC.2022.v38i1.522","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Traumatic brain injury (TBI) is a common cause of paediatric intensive care unit (PICU) admissions in South Africa. Optimal care of these patients includes the prevention and control of post-traumatic seizures (PTS) in order to minimise secondary brain injury.</p><p><strong>Objectives: </strong>To describe the demographics of children admitted to a South African PICU, to describe the characteristics of PTS, and to describe the prophylactic and therapeutic management of PTS within the unit.</p><p><strong>Methods: </strong>A 3-year retrospective chart review was conducted at the PICU of the Chris Hani Baragwanath Academic Hospital (CHBAH) in Soweto, Johannesburg, from 1 July 2015 to 30 June 2018.</p><p><strong>Results: </strong>Seventy-eight patients were admitted to the PICU, all with severe TBI. A total of 66 patient files were available for analysis. The median age of admission was 6 years (interquartile range (IQR) 4 - 9) with the majority of trauma secondary to mechanical injury (89%). Prophylactic anti-epileptic drugs (AEDs) were initiated in 44 (79%) patients. Early PTS occurred in 11 (25%) patients who received prophylaxis and 4 (33%) who did not. Three (5%) patients developed late PTS, resulting in an overall incidence of PTS of 43%. The most common seizure type was generalised tonic clonic (82%). Children diagnosed with PTS were a median of 2 years younger than those without PTS, with increased prevalence of seizures (83% v. 38%) in children below 2 years of age. Maintenance therapy was initiated in all patients consistent with recommended dosages. Of the total 167 anti-epileptic levels taken during maintenance, only 56% were within target range. Of the initial 78 patients, 8 died (10%). The median length of stay was 7 (IQR 5 - 12) and 8 (IQR 8 - 24) days longer in ICU and hospital respectively, in children with PTS.</p><p><strong>Conclusion: </strong>PTS is a frequent complication of severe TBI in children. There was considerable variation in the approach to both prophylaxis and maintenance therapy of PTS in terms of choice of agent, dosage, frequency of drug monitoring and approach to subtherapeutic levels. It is clear that more high-level studies are required in order to better inform these practices.</p><p><strong>Contributions of the study: </strong>To the best of our knowledge, this article represents the first description of incidence and management practices of paediatric post traumatic seizures.</p>","PeriodicalId":75194,"journal":{"name":"The Southern African journal of critical care : the official journal of the Critical Care Society","volume":" ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2022-05-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b5/3a/SAJCC-38-1-522.PMC9275334.pdf","citationCount":"0","resultStr":"{\"title\":\"Pharmacological management of post-traumatic seizures in a South African paediatric intensive care unit.\",\"authors\":\"N Yachad, K D Naidoo\",\"doi\":\"10.7196/SAJCC.2022.v38i1.522\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Traumatic brain injury (TBI) is a common cause of paediatric intensive care unit (PICU) admissions in South Africa. Optimal care of these patients includes the prevention and control of post-traumatic seizures (PTS) in order to minimise secondary brain injury.</p><p><strong>Objectives: </strong>To describe the demographics of children admitted to a South African PICU, to describe the characteristics of PTS, and to describe the prophylactic and therapeutic management of PTS within the unit.</p><p><strong>Methods: </strong>A 3-year retrospective chart review was conducted at the PICU of the Chris Hani Baragwanath Academic Hospital (CHBAH) in Soweto, Johannesburg, from 1 July 2015 to 30 June 2018.</p><p><strong>Results: </strong>Seventy-eight patients were admitted to the PICU, all with severe TBI. A total of 66 patient files were available for analysis. The median age of admission was 6 years (interquartile range (IQR) 4 - 9) with the majority of trauma secondary to mechanical injury (89%). Prophylactic anti-epileptic drugs (AEDs) were initiated in 44 (79%) patients. Early PTS occurred in 11 (25%) patients who received prophylaxis and 4 (33%) who did not. Three (5%) patients developed late PTS, resulting in an overall incidence of PTS of 43%. The most common seizure type was generalised tonic clonic (82%). Children diagnosed with PTS were a median of 2 years younger than those without PTS, with increased prevalence of seizures (83% v. 38%) in children below 2 years of age. Maintenance therapy was initiated in all patients consistent with recommended dosages. Of the total 167 anti-epileptic levels taken during maintenance, only 56% were within target range. Of the initial 78 patients, 8 died (10%). The median length of stay was 7 (IQR 5 - 12) and 8 (IQR 8 - 24) days longer in ICU and hospital respectively, in children with PTS.</p><p><strong>Conclusion: </strong>PTS is a frequent complication of severe TBI in children. There was considerable variation in the approach to both prophylaxis and maintenance therapy of PTS in terms of choice of agent, dosage, frequency of drug monitoring and approach to subtherapeutic levels. It is clear that more high-level studies are required in order to better inform these practices.</p><p><strong>Contributions of the study: </strong>To the best of our knowledge, this article represents the first description of incidence and management practices of paediatric post traumatic seizures.</p>\",\"PeriodicalId\":75194,\"journal\":{\"name\":\"The Southern African journal of critical care : the official journal of the Critical Care Society\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-05-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b5/3a/SAJCC-38-1-522.PMC9275334.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Southern African journal of critical care : the official journal of the Critical Care Society\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.7196/SAJCC.2022.v38i1.522\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Southern African journal of critical care : the official journal of the Critical Care Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7196/SAJCC.2022.v38i1.522","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Pharmacological management of post-traumatic seizures in a South African paediatric intensive care unit.
Background: Traumatic brain injury (TBI) is a common cause of paediatric intensive care unit (PICU) admissions in South Africa. Optimal care of these patients includes the prevention and control of post-traumatic seizures (PTS) in order to minimise secondary brain injury.
Objectives: To describe the demographics of children admitted to a South African PICU, to describe the characteristics of PTS, and to describe the prophylactic and therapeutic management of PTS within the unit.
Methods: A 3-year retrospective chart review was conducted at the PICU of the Chris Hani Baragwanath Academic Hospital (CHBAH) in Soweto, Johannesburg, from 1 July 2015 to 30 June 2018.
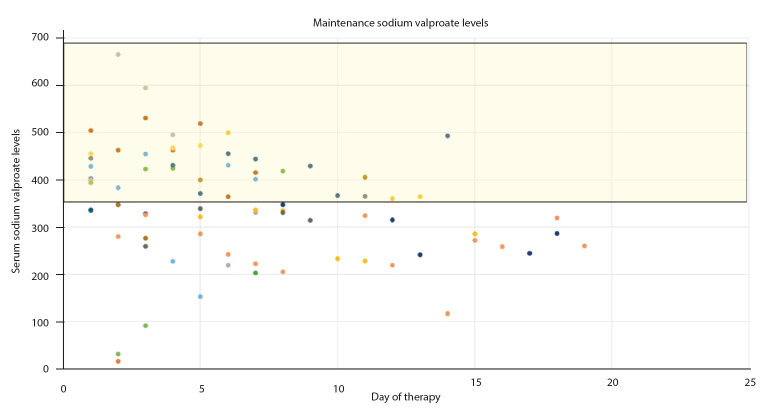
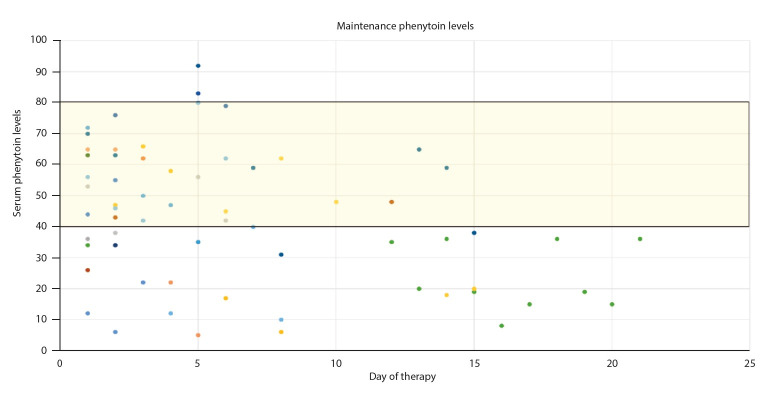
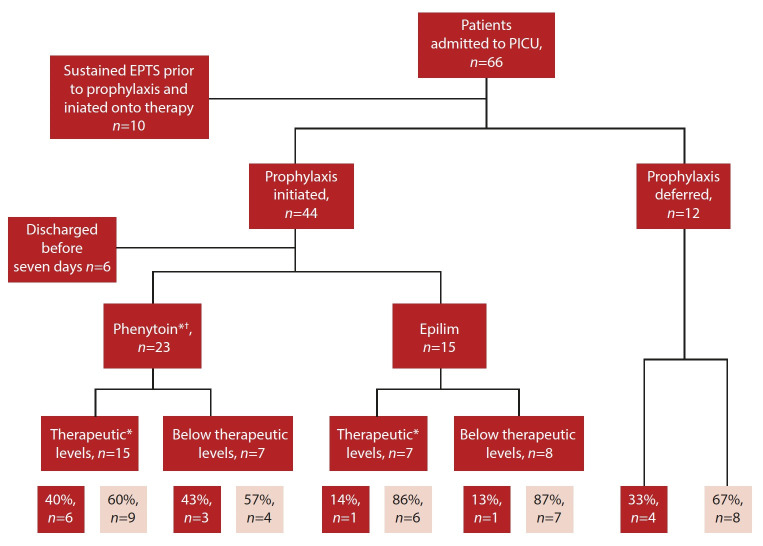
Results: Seventy-eight patients were admitted to the PICU, all with severe TBI. A total of 66 patient files were available for analysis. The median age of admission was 6 years (interquartile range (IQR) 4 - 9) with the majority of trauma secondary to mechanical injury (89%). Prophylactic anti-epileptic drugs (AEDs) were initiated in 44 (79%) patients. Early PTS occurred in 11 (25%) patients who received prophylaxis and 4 (33%) who did not. Three (5%) patients developed late PTS, resulting in an overall incidence of PTS of 43%. The most common seizure type was generalised tonic clonic (82%). Children diagnosed with PTS were a median of 2 years younger than those without PTS, with increased prevalence of seizures (83% v. 38%) in children below 2 years of age. Maintenance therapy was initiated in all patients consistent with recommended dosages. Of the total 167 anti-epileptic levels taken during maintenance, only 56% were within target range. Of the initial 78 patients, 8 died (10%). The median length of stay was 7 (IQR 5 - 12) and 8 (IQR 8 - 24) days longer in ICU and hospital respectively, in children with PTS.
Conclusion: PTS is a frequent complication of severe TBI in children. There was considerable variation in the approach to both prophylaxis and maintenance therapy of PTS in terms of choice of agent, dosage, frequency of drug monitoring and approach to subtherapeutic levels. It is clear that more high-level studies are required in order to better inform these practices.
Contributions of the study: To the best of our knowledge, this article represents the first description of incidence and management practices of paediatric post traumatic seizures.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


