{"title":"危重病人的评分系统:哪一个用于癌症患者?","authors":"Anisha Beniwal, Deven Juneja, Omender Singh, Amit Goel, Akhilesh Singh, Hemant Kumar Beniwal","doi":"10.5492/wjccm.v11.i6.364","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Scoring systems have not been evaluated in oncology patients. We aimed to assess the performance of Acute Physiology and Chronic Health Evaluation (APACHE) II, APACHE III, APACHE IV, Simplified Acute Physiology Score (SAPS) II, SAPS III, Mortality Probability Model (MPM) II<sub>0</sub> and Sequential Organ Failure Assessment (SOFA) score in critically ill oncology patients.</p><p><strong>Aim: </strong>To compare the efficacy of seven commonly employed scoring systems to predict outcomes of critically ill cancer patients.</p><p><strong>Methods: </strong>We conducted a retrospective analysis of 400 consecutive cancer patients admitted in the medical intensive care unit over a two-year period. Primary outcome was hospital mortality and the secondary outcome measure was comparison of various scoring systems in predicting hospital mortality.</p><p><strong>Results: </strong>In our study, the overall intensive care unit and hospital mortality was 43.5% and 57.8%, respectively. All of the seven tested scores underestimated mortality. The mortality as predicted by MPM II<sub>0</sub> predicted death rate (PDR) was nearest to the actual mortality followed by that predicted by APACHE II, with a standardized mortality rate (SMR) of 1.305 and 1.547, respectively. The best calibration was shown by the APACHE III score (<i>χ</i> <sup>2</sup> = 4.704, <i>P</i> = 0.788). On the other hand, SOFA score (<i>χ</i> <sup>2</sup> = 15.966, <i>P</i> = 0.025) had the worst calibration, although the difference was not statistically significant. All of the seven scores had acceptable discrimination with good efficacy however, SAPS III PDR and MPM II<sub>0</sub> PDR (AUROC = 0.762), had a better performance as compared to others. The correlation between the different scoring systems was significant (<i>P</i> < 0.001).</p><p><strong>Conclusion: </strong>All the severity scores were tested under-predicted mortality in the present study. As the difference in efficacy and performance was not statistically significant, the choice of scoring system used may depend on the ease of use and local preferences.</p>","PeriodicalId":66959,"journal":{"name":"世界危重病急救学杂志(英文版)","volume":"11 6","pages":"364-374"},"PeriodicalIF":0.0000,"publicationDate":"2022-11-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6a/36/WJCCM-11-364.PMC9693908.pdf","citationCount":"0","resultStr":"{\"title\":\"Scoring systems in critically ill: Which one to use in cancer patients?\",\"authors\":\"Anisha Beniwal, Deven Juneja, Omender Singh, Amit Goel, Akhilesh Singh, Hemant Kumar Beniwal\",\"doi\":\"10.5492/wjccm.v11.i6.364\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Scoring systems have not been evaluated in oncology patients. We aimed to assess the performance of Acute Physiology and Chronic Health Evaluation (APACHE) II, APACHE III, APACHE IV, Simplified Acute Physiology Score (SAPS) II, SAPS III, Mortality Probability Model (MPM) II<sub>0</sub> and Sequential Organ Failure Assessment (SOFA) score in critically ill oncology patients.</p><p><strong>Aim: </strong>To compare the efficacy of seven commonly employed scoring systems to predict outcomes of critically ill cancer patients.</p><p><strong>Methods: </strong>We conducted a retrospective analysis of 400 consecutive cancer patients admitted in the medical intensive care unit over a two-year period. Primary outcome was hospital mortality and the secondary outcome measure was comparison of various scoring systems in predicting hospital mortality.</p><p><strong>Results: </strong>In our study, the overall intensive care unit and hospital mortality was 43.5% and 57.8%, respectively. All of the seven tested scores underestimated mortality. The mortality as predicted by MPM II<sub>0</sub> predicted death rate (PDR) was nearest to the actual mortality followed by that predicted by APACHE II, with a standardized mortality rate (SMR) of 1.305 and 1.547, respectively. The best calibration was shown by the APACHE III score (<i>χ</i> <sup>2</sup> = 4.704, <i>P</i> = 0.788). On the other hand, SOFA score (<i>χ</i> <sup>2</sup> = 15.966, <i>P</i> = 0.025) had the worst calibration, although the difference was not statistically significant. All of the seven scores had acceptable discrimination with good efficacy however, SAPS III PDR and MPM II<sub>0</sub> PDR (AUROC = 0.762), had a better performance as compared to others. The correlation between the different scoring systems was significant (<i>P</i> < 0.001).</p><p><strong>Conclusion: </strong>All the severity scores were tested under-predicted mortality in the present study. As the difference in efficacy and performance was not statistically significant, the choice of scoring system used may depend on the ease of use and local preferences.</p>\",\"PeriodicalId\":66959,\"journal\":{\"name\":\"世界危重病急救学杂志(英文版)\",\"volume\":\"11 6\",\"pages\":\"364-374\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-11-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6a/36/WJCCM-11-364.PMC9693908.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"世界危重病急救学杂志(英文版)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5492/wjccm.v11.i6.364\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界危重病急救学杂志(英文版)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5492/wjccm.v11.i6.364","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:评分系统尚未在肿瘤患者中进行评估。我们的目的是评估急性生理和慢性健康评估(APACHE) II, APACHE III, APACHE IV,简化急性生理评分(SAPS) II, SAPS III,死亡率概率模型(MPM) II0和顺序器官衰竭评估(SOFA)评分在危重肿瘤患者中的表现。目的:比较7种常用评分系统对危重癌症患者预后的预测效果。方法:我们对两年多来在重症监护病房连续住院的400例癌症患者进行了回顾性分析。主要结果是医院死亡率,次要结果测量是预测医院死亡率的各种评分系统的比较。结果:本组重症监护病房死亡率43.5%,住院死亡率57.8%。所有七个测试分数都低估了死亡率。MPM II0预测死亡率(PDR)预测的死亡率最接近实际,其次是APACHE II预测的标准化死亡率(SMR),分别为1.305和1.547。APACHE III评分显示最佳校准(χ 2 = 4.704, P = 0.788)。另一方面,SOFA评分(χ 2 = 15.966, P = 0.025)的校正效果最差,但差异无统计学意义。7种评分均具有可接受的区分性,且均有较好的疗效,但以SAPS III PDR和MPM II0 PDR (AUROC = 0.762)表现较好。不同评分系统间相关性显著(P < 0.001)。结论:本研究中所有严重程度评分均低于预测死亡率。由于疗效和表现的差异没有统计学意义,因此使用评分系统的选择可能取决于易用性和当地偏好。
Scoring systems in critically ill: Which one to use in cancer patients?
Background: Scoring systems have not been evaluated in oncology patients. We aimed to assess the performance of Acute Physiology and Chronic Health Evaluation (APACHE) II, APACHE III, APACHE IV, Simplified Acute Physiology Score (SAPS) II, SAPS III, Mortality Probability Model (MPM) II0 and Sequential Organ Failure Assessment (SOFA) score in critically ill oncology patients.
Aim: To compare the efficacy of seven commonly employed scoring systems to predict outcomes of critically ill cancer patients.
Methods: We conducted a retrospective analysis of 400 consecutive cancer patients admitted in the medical intensive care unit over a two-year period. Primary outcome was hospital mortality and the secondary outcome measure was comparison of various scoring systems in predicting hospital mortality.
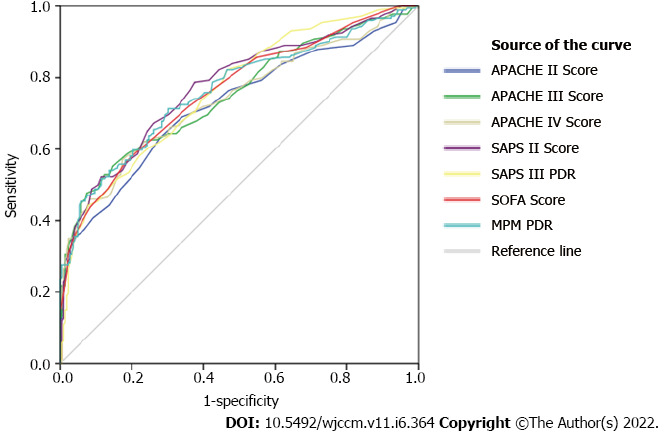
Results: In our study, the overall intensive care unit and hospital mortality was 43.5% and 57.8%, respectively. All of the seven tested scores underestimated mortality. The mortality as predicted by MPM II0 predicted death rate (PDR) was nearest to the actual mortality followed by that predicted by APACHE II, with a standardized mortality rate (SMR) of 1.305 and 1.547, respectively. The best calibration was shown by the APACHE III score (χ2 = 4.704, P = 0.788). On the other hand, SOFA score (χ2 = 15.966, P = 0.025) had the worst calibration, although the difference was not statistically significant. All of the seven scores had acceptable discrimination with good efficacy however, SAPS III PDR and MPM II0 PDR (AUROC = 0.762), had a better performance as compared to others. The correlation between the different scoring systems was significant (P < 0.001).
Conclusion: All the severity scores were tested under-predicted mortality in the present study. As the difference in efficacy and performance was not statistically significant, the choice of scoring system used may depend on the ease of use and local preferences.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


