{"title":"伊马替尼耐药胃肠道间质瘤综述。","authors":"Yujiro Hayashi, Vy Truong Thuy Nguyen","doi":"10.21037/gist-21-10","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Review the studies that investigate the mechanisms underlying imatinib-resistant gastrointestinal stromal tumors (GIST).</p><p><strong>Background: </strong>GIST are the most common mesenchymal tumors of the gastrointestinal (GI) tract and the most common sarcoma in humans. GIST are thought to be arise from interstitial cells of Cajal (ICC), pacemaker and neuromodulator cells in the GI tract, as well as \"fibroblast\"-like cells, which are another type of interstitial cells of the gut wall and also known as telocyte or platelet-derived growth factor-alpha (PDGFRA)-positive cells. The majority of GIST harbor gain-of-function mutations in either <i>KIT</i> or <i>PDGFRA</i>, and these gain-of-function mutations are mutually exclusive and most often heterozygous. GIST are responsive to the KIT/PDGFRA tyrosine kinase inhibitor (TKI), imatinib, the standard first-line drug for advanced and metastatic GIST. However, imatinib alone does not eradicate GIST despite an initial clinical benefit, and more than 90% of GIST harbor imatinib-resistance. Although second and third-generation TKIs have been developed and are currently in clinical use, they are not curative for refractory and metastatic GIST due to the emergence of clones with drug-resistant mutations. Eradication of drug-resistant GIST will cure patients with refractory GIST. Several mechanisms may contribute to refractory GIST. These mechanisms are secondary mutations in <i>KIT</i> and/or <i>PDGFRA</i>, alternative activation of tyrosine kinases, stem cells for GIST and cellular quiescence, a reversible nonproliferating state in which cells retain the ability to reenter cell proliferation.</p><p><strong>Methods: </strong>We review our current optimal treatment approach for managing patients with advanced and refractory GIST.</p><p><strong>Conclusions: </strong>This review explores the novel and potential therapeutic approaches to combat drug-resistant GIST.</p>","PeriodicalId":93755,"journal":{"name":"Gastrointestinal stromal tumor","volume":"4 ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2021-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/69/d7/nihms-1767211.PMC9268655.pdf","citationCount":"0","resultStr":"{\"title\":\"A narrative review of imatinib-resistant gastrointestinal stromal tumors.\",\"authors\":\"Yujiro Hayashi, Vy Truong Thuy Nguyen\",\"doi\":\"10.21037/gist-21-10\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Review the studies that investigate the mechanisms underlying imatinib-resistant gastrointestinal stromal tumors (GIST).</p><p><strong>Background: </strong>GIST are the most common mesenchymal tumors of the gastrointestinal (GI) tract and the most common sarcoma in humans. GIST are thought to be arise from interstitial cells of Cajal (ICC), pacemaker and neuromodulator cells in the GI tract, as well as \\\"fibroblast\\\"-like cells, which are another type of interstitial cells of the gut wall and also known as telocyte or platelet-derived growth factor-alpha (PDGFRA)-positive cells. The majority of GIST harbor gain-of-function mutations in either <i>KIT</i> or <i>PDGFRA</i>, and these gain-of-function mutations are mutually exclusive and most often heterozygous. GIST are responsive to the KIT/PDGFRA tyrosine kinase inhibitor (TKI), imatinib, the standard first-line drug for advanced and metastatic GIST. However, imatinib alone does not eradicate GIST despite an initial clinical benefit, and more than 90% of GIST harbor imatinib-resistance. Although second and third-generation TKIs have been developed and are currently in clinical use, they are not curative for refractory and metastatic GIST due to the emergence of clones with drug-resistant mutations. Eradication of drug-resistant GIST will cure patients with refractory GIST. Several mechanisms may contribute to refractory GIST. These mechanisms are secondary mutations in <i>KIT</i> and/or <i>PDGFRA</i>, alternative activation of tyrosine kinases, stem cells for GIST and cellular quiescence, a reversible nonproliferating state in which cells retain the ability to reenter cell proliferation.</p><p><strong>Methods: </strong>We review our current optimal treatment approach for managing patients with advanced and refractory GIST.</p><p><strong>Conclusions: </strong>This review explores the novel and potential therapeutic approaches to combat drug-resistant GIST.</p>\",\"PeriodicalId\":93755,\"journal\":{\"name\":\"Gastrointestinal stromal tumor\",\"volume\":\"4 \",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/69/d7/nihms-1767211.PMC9268655.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Gastrointestinal stromal tumor\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.21037/gist-21-10\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/10/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gastrointestinal stromal tumor","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/gist-21-10","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/10/30 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
A narrative review of imatinib-resistant gastrointestinal stromal tumors.
Objective: Review the studies that investigate the mechanisms underlying imatinib-resistant gastrointestinal stromal tumors (GIST).
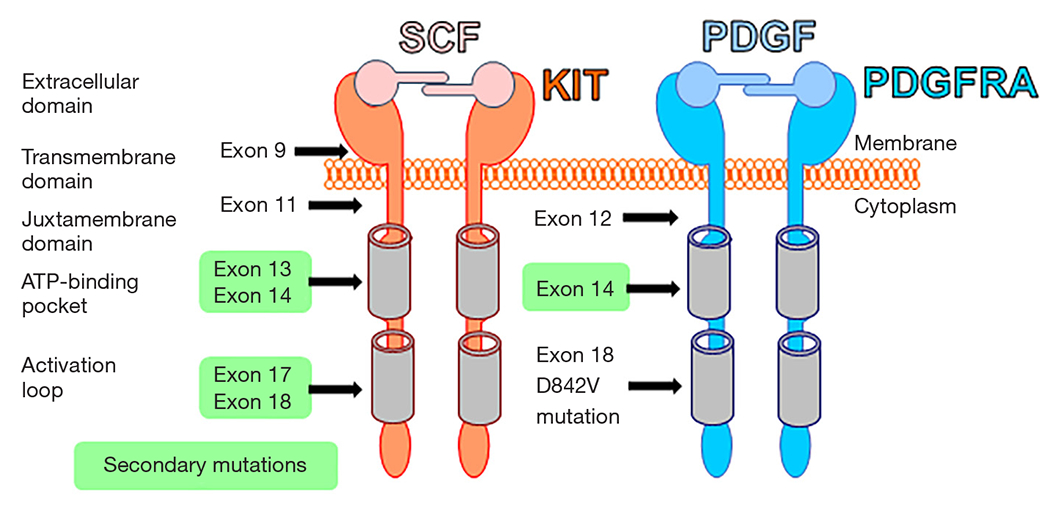
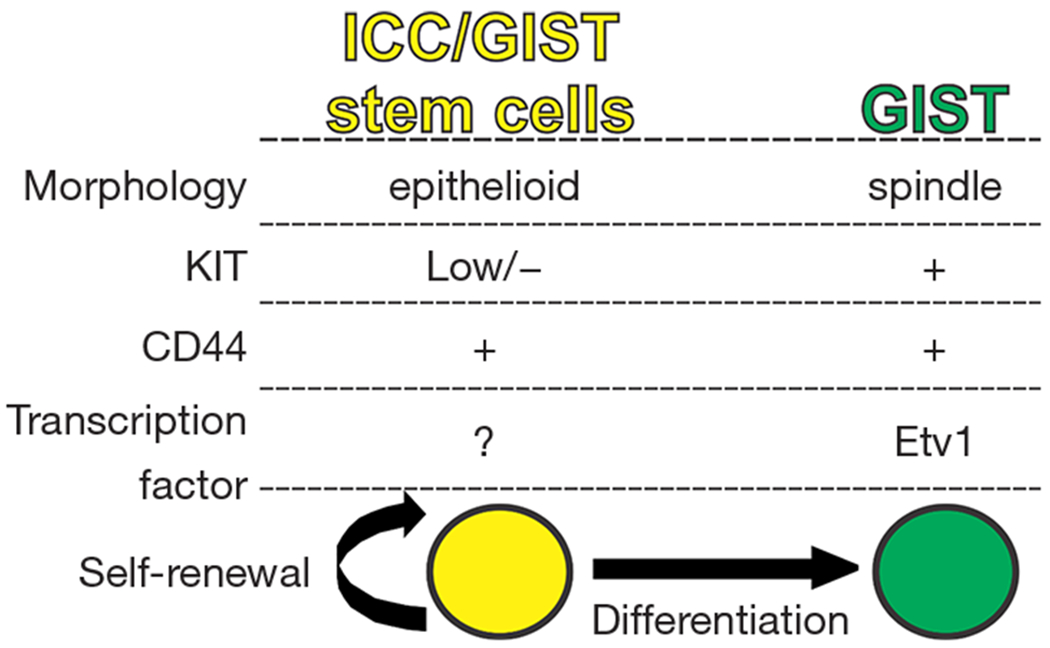
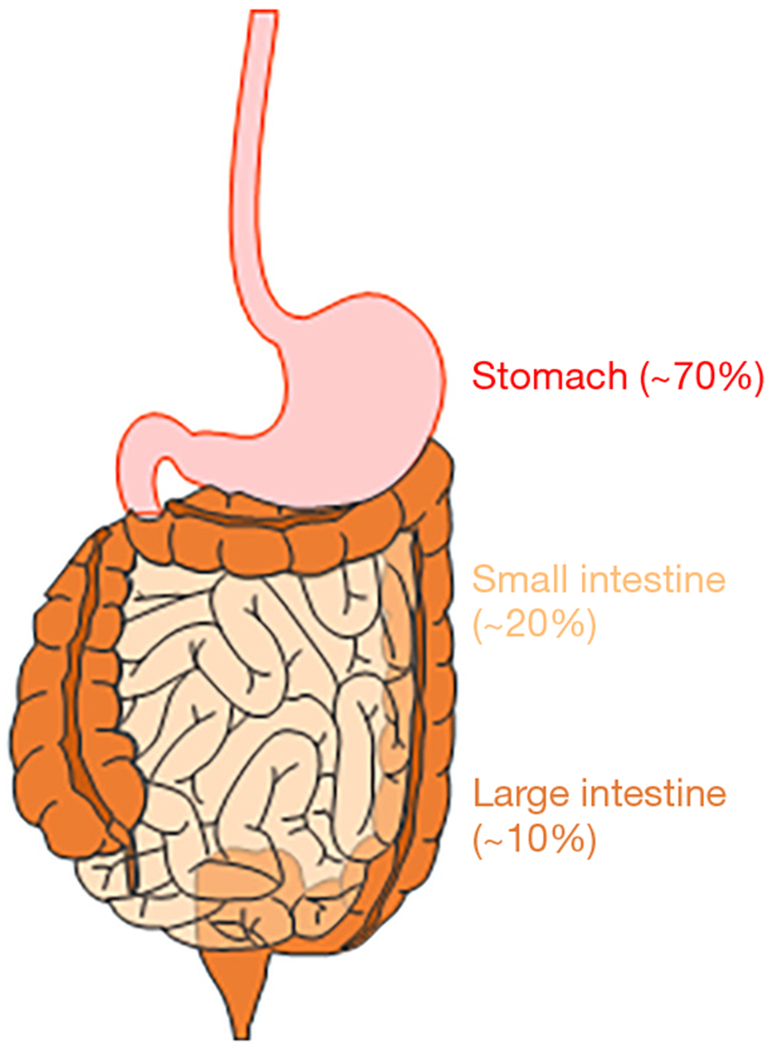
Background: GIST are the most common mesenchymal tumors of the gastrointestinal (GI) tract and the most common sarcoma in humans. GIST are thought to be arise from interstitial cells of Cajal (ICC), pacemaker and neuromodulator cells in the GI tract, as well as "fibroblast"-like cells, which are another type of interstitial cells of the gut wall and also known as telocyte or platelet-derived growth factor-alpha (PDGFRA)-positive cells. The majority of GIST harbor gain-of-function mutations in either KIT or PDGFRA, and these gain-of-function mutations are mutually exclusive and most often heterozygous. GIST are responsive to the KIT/PDGFRA tyrosine kinase inhibitor (TKI), imatinib, the standard first-line drug for advanced and metastatic GIST. However, imatinib alone does not eradicate GIST despite an initial clinical benefit, and more than 90% of GIST harbor imatinib-resistance. Although second and third-generation TKIs have been developed and are currently in clinical use, they are not curative for refractory and metastatic GIST due to the emergence of clones with drug-resistant mutations. Eradication of drug-resistant GIST will cure patients with refractory GIST. Several mechanisms may contribute to refractory GIST. These mechanisms are secondary mutations in KIT and/or PDGFRA, alternative activation of tyrosine kinases, stem cells for GIST and cellular quiescence, a reversible nonproliferating state in which cells retain the ability to reenter cell proliferation.
Methods: We review our current optimal treatment approach for managing patients with advanced and refractory GIST.
Conclusions: This review explores the novel and potential therapeutic approaches to combat drug-resistant GIST.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


