{"title":"胸椎手术后带状疱疹介导的神经根炎。","authors":"Hyo Sae Ahn, Doo Hyuk Kwon","doi":"10.3988/jcn.2022.18.4.484","DOIUrl":null,"url":null,"abstract":"Dear Editor, Varicella zoster virus (VZV) primarily infects children and reactivates in adulthood, causing herpes zoster (also called shingles). Herpes zoster induces pain along the skin dermatome that is accompanied by characteristic band-shaped blisters. Known risk factors include infection with human immunodeficiency virus, bone marrow transplantation, leukemia, lymphoma, receiving immunosuppressors including chemotherapy or steroids, various autoimmune diseases, old age, trauma, female sex, asthma, diabetes, and chronic obstructive pulmonary disease.1,2 In cases of spinal diseases, VZV can be reactivated after interventions including injection therapy or various surgical treatments, including spinal surgery.3-5 However, herpes zoster is quite rare in clinical neurology. A 53-year-old male patient visited the emergency room with a chief complaint of weakness in both legs that started 3 days prior without any history of trauma. He had liver cirrhosis. On neurological examination, the strength of both lower limbs was Medical Research Council scale grade 1, and there was no sensation at all. On thoracolumbar spine magnetic resonance imaging revealed right T1–T2 paracentral disc herniation with cord compression and cord signal change (Fig. 1A and B). The patient was diagnosed with thoracic myelopathy. The following surgical treatment was performed immediately: T1 total laminectomy, C7 and T2 dome laminoplasty, T1–T2 discectomy, and T1–T2 postfusion with a pedicle screw (Fig. 1C and D). After surgical treatment, the muscle strength and sensation in the lower limbs gradually improved. However, 10 days after the operation, the patient complained of a stinging sensation on the right chest wall and upper arm associated with vesicular skin rashes (Fig. 1E and F) that had developed along the right T1 dermatome, which were compatible with herpes zoster viral infection. Valacyclovir (1 g) was administered orally three times a day for 7 days, and the stinging symptoms and skin rash subsequently improved. In this case, herpes zoster occurred in the related segment (T1 dermatome) after surgical treatment for thoracic myelopathy caused by right T1–T2 paracentral disc herniation. The exact mechanism of VZV reactivation remains unknown. Reactivation of the VZV under reduced virus-specific cell-mediated immune responses induces widespread cell-to-cell proliferation, strong local inflammatory responses, and widespread necrosis of neuroglial cells and neurons within the ganglion. VZV spreads down the sensory nerve and is then released from the nerve endings in the skin, causing a cutaneous dermatomal rash.6 Although it is unclear how local surgical trauma can reactivate VZV in the ganglion,6,7 we hypothesized that the reactivation was due to a decline in VZV-specific cell-mediated immunity and disruption of cutaneous immunity caused by stimulating the sensory nerve. General anesthesia and surgeryrelated stress can reduce virus-specific cell-mediated immune responses.1,6,7 Direct pressure on the ganglion by root manipulation during surgery stimulates sensory nerves, which can disrupt local cutaneous immunity.1,8 The timing of symptoms after the inciting event varies, Hyo Sae Ahn Doo Hyuk Kwon","PeriodicalId":324902,"journal":{"name":"Journal of Clinical Neurology (Seoul, Korea)","volume":" ","pages":"484-486"},"PeriodicalIF":0.0000,"publicationDate":"2022-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a0/e5/jcn-18-484.PMC9262449.pdf","citationCount":"0","resultStr":"{\"title\":\"Herpes-Zoster-Mediated Radiculitis After Thoracic Spine Surgery.\",\"authors\":\"Hyo Sae Ahn, Doo Hyuk Kwon\",\"doi\":\"10.3988/jcn.2022.18.4.484\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Dear Editor, Varicella zoster virus (VZV) primarily infects children and reactivates in adulthood, causing herpes zoster (also called shingles). Herpes zoster induces pain along the skin dermatome that is accompanied by characteristic band-shaped blisters. Known risk factors include infection with human immunodeficiency virus, bone marrow transplantation, leukemia, lymphoma, receiving immunosuppressors including chemotherapy or steroids, various autoimmune diseases, old age, trauma, female sex, asthma, diabetes, and chronic obstructive pulmonary disease.1,2 In cases of spinal diseases, VZV can be reactivated after interventions including injection therapy or various surgical treatments, including spinal surgery.3-5 However, herpes zoster is quite rare in clinical neurology. A 53-year-old male patient visited the emergency room with a chief complaint of weakness in both legs that started 3 days prior without any history of trauma. He had liver cirrhosis. On neurological examination, the strength of both lower limbs was Medical Research Council scale grade 1, and there was no sensation at all. On thoracolumbar spine magnetic resonance imaging revealed right T1–T2 paracentral disc herniation with cord compression and cord signal change (Fig. 1A and B). The patient was diagnosed with thoracic myelopathy. The following surgical treatment was performed immediately: T1 total laminectomy, C7 and T2 dome laminoplasty, T1–T2 discectomy, and T1–T2 postfusion with a pedicle screw (Fig. 1C and D). After surgical treatment, the muscle strength and sensation in the lower limbs gradually improved. However, 10 days after the operation, the patient complained of a stinging sensation on the right chest wall and upper arm associated with vesicular skin rashes (Fig. 1E and F) that had developed along the right T1 dermatome, which were compatible with herpes zoster viral infection. Valacyclovir (1 g) was administered orally three times a day for 7 days, and the stinging symptoms and skin rash subsequently improved. In this case, herpes zoster occurred in the related segment (T1 dermatome) after surgical treatment for thoracic myelopathy caused by right T1–T2 paracentral disc herniation. The exact mechanism of VZV reactivation remains unknown. Reactivation of the VZV under reduced virus-specific cell-mediated immune responses induces widespread cell-to-cell proliferation, strong local inflammatory responses, and widespread necrosis of neuroglial cells and neurons within the ganglion. VZV spreads down the sensory nerve and is then released from the nerve endings in the skin, causing a cutaneous dermatomal rash.6 Although it is unclear how local surgical trauma can reactivate VZV in the ganglion,6,7 we hypothesized that the reactivation was due to a decline in VZV-specific cell-mediated immunity and disruption of cutaneous immunity caused by stimulating the sensory nerve. General anesthesia and surgeryrelated stress can reduce virus-specific cell-mediated immune responses.1,6,7 Direct pressure on the ganglion by root manipulation during surgery stimulates sensory nerves, which can disrupt local cutaneous immunity.1,8 The timing of symptoms after the inciting event varies, Hyo Sae Ahn Doo Hyuk Kwon\",\"PeriodicalId\":324902,\"journal\":{\"name\":\"Journal of Clinical Neurology (Seoul, Korea)\",\"volume\":\" \",\"pages\":\"484-486\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a0/e5/jcn-18-484.PMC9262449.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Neurology (Seoul, Korea)\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3988/jcn.2022.18.4.484\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Neurology (Seoul, Korea)","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3988/jcn.2022.18.4.484","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Herpes-Zoster-Mediated Radiculitis After Thoracic Spine Surgery.
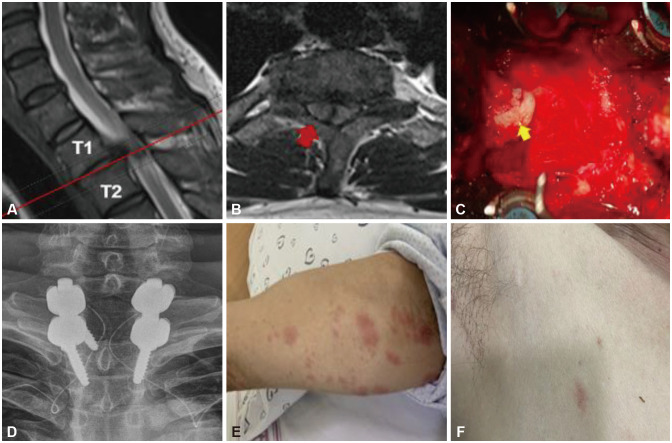
Dear Editor, Varicella zoster virus (VZV) primarily infects children and reactivates in adulthood, causing herpes zoster (also called shingles). Herpes zoster induces pain along the skin dermatome that is accompanied by characteristic band-shaped blisters. Known risk factors include infection with human immunodeficiency virus, bone marrow transplantation, leukemia, lymphoma, receiving immunosuppressors including chemotherapy or steroids, various autoimmune diseases, old age, trauma, female sex, asthma, diabetes, and chronic obstructive pulmonary disease.1,2 In cases of spinal diseases, VZV can be reactivated after interventions including injection therapy or various surgical treatments, including spinal surgery.3-5 However, herpes zoster is quite rare in clinical neurology. A 53-year-old male patient visited the emergency room with a chief complaint of weakness in both legs that started 3 days prior without any history of trauma. He had liver cirrhosis. On neurological examination, the strength of both lower limbs was Medical Research Council scale grade 1, and there was no sensation at all. On thoracolumbar spine magnetic resonance imaging revealed right T1–T2 paracentral disc herniation with cord compression and cord signal change (Fig. 1A and B). The patient was diagnosed with thoracic myelopathy. The following surgical treatment was performed immediately: T1 total laminectomy, C7 and T2 dome laminoplasty, T1–T2 discectomy, and T1–T2 postfusion with a pedicle screw (Fig. 1C and D). After surgical treatment, the muscle strength and sensation in the lower limbs gradually improved. However, 10 days after the operation, the patient complained of a stinging sensation on the right chest wall and upper arm associated with vesicular skin rashes (Fig. 1E and F) that had developed along the right T1 dermatome, which were compatible with herpes zoster viral infection. Valacyclovir (1 g) was administered orally three times a day for 7 days, and the stinging symptoms and skin rash subsequently improved. In this case, herpes zoster occurred in the related segment (T1 dermatome) after surgical treatment for thoracic myelopathy caused by right T1–T2 paracentral disc herniation. The exact mechanism of VZV reactivation remains unknown. Reactivation of the VZV under reduced virus-specific cell-mediated immune responses induces widespread cell-to-cell proliferation, strong local inflammatory responses, and widespread necrosis of neuroglial cells and neurons within the ganglion. VZV spreads down the sensory nerve and is then released from the nerve endings in the skin, causing a cutaneous dermatomal rash.6 Although it is unclear how local surgical trauma can reactivate VZV in the ganglion,6,7 we hypothesized that the reactivation was due to a decline in VZV-specific cell-mediated immunity and disruption of cutaneous immunity caused by stimulating the sensory nerve. General anesthesia and surgeryrelated stress can reduce virus-specific cell-mediated immune responses.1,6,7 Direct pressure on the ganglion by root manipulation during surgery stimulates sensory nerves, which can disrupt local cutaneous immunity.1,8 The timing of symptoms after the inciting event varies, Hyo Sae Ahn Doo Hyuk Kwon

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


