So Hyun Yim, Jae Seob Yoon, Chang Hun Lee, Jiyoung Kim
{"title":"igg4相关疾病中的增生性厚性脑膜炎和间质性肺疾病。","authors":"So Hyun Yim, Jae Seob Yoon, Chang Hun Lee, Jiyoung Kim","doi":"10.3988/jcn.2022.18.4.481","DOIUrl":null,"url":null,"abstract":"Dear Editor, IgG4-related disease (IgG4-RD) is an immune-mediated inflammatory condition characterized by elevated serum IgG4 and affected organs being infiltrated by IgG4-positive plasma cells.1 This disease can affect multiple organs, but rarely involves the central nervous system (CNS).2 Here we report a case of IgG4-RD presenting as hypertrophic pachymeningitis (HP), which was confirmed in a lung biopsy. A 57-year-old female presented to our hospital with a throbbing headache that began 1 year previously. The pain persisted in the entire head and was more severe on the right side; the patient also had interstitial lung disease (ILD) (Fig. 1A). Although the patient did not present with joint tenderness, the presence of rheumatoid arthritis was supported by elevated C-reactive protein and an increased erythrocyte sedimentation rate. She had been prescribed methylprednisolone (2 mg/day) and tacrolimus (0.5 mg/day) for rheumatoid arthritis. Brain magnetic resonance imaging (MRI) performed in another hospital 5 months previously did not detect any structural lesions that could explain the headache symptoms (Fig. 1B). The patient had been diagnosed with chronic migraine at that time. Despite taking both acute and preventive migraine medications for 5 months, the headache became more severe and interfered with her daily physical activities and the quality of sleep at nighttime. Brain MRI performed upon admission to our hospital revealed pachymeningeal thickening with enhancement in the right hemisphere (Fig. 1C), which had not been found in the previous MRI. An examination of the CSF revealed slight elevation of the WBC count (12/μL, lymphocyte-dominant), whereas protein (37.2 mg/dL) and glucose (66.0 mg/dL) levels were within the normal ranges. Attributing the headaches to IgG4-RD was considered based on the HP revealed by brain MRI and the ILD comorbidity. We investigated the patient’s serum for subclasses of IgG, and found elevated IgG4 (186.4 mg/dL, reference range: 3.9–86.4 mg/dL). A lung biopsy was performed to confirm the diagnosis, because it is safer and easier than a meningeal biopsy. The lung biopsy revealed obliteration of venular vessels and storiform fibrosis with infiltration by lymphoplasma cells (Fig. 1E and F). IgG and IgG4 were found in plasma cells by immunohistochemistry (Fig. 1G and H). Based on the clinical and radiological features observed and the serological and pathological findings, the patient was diagnosed with IgG4-RD.3 She was treated with a high dose of prednisolone (1,000 mg/day for 5 days), followed by rituximab (375 mg/m2). Subsequent MRI revealed decreased pachymeningeal enhancement (Fig. 1D). IgG4-RD can affect various organs, and in this case two organs were involved: the lungs and the brain. The most commonly affected body parts include the pancreas, salivary and lacrimal glands, biliary tract, thyroid, kidney, and lung, while the CNS is rarely involved.4 Diseases that can affect each of these organs are type 1 autoimmune pancreatitis, Mikulicz disease, IgGrelated sclerosing cholangitis, and Riedel’s thyroiditis, and their common clinical, laboratory, and histological features have led to them being classified into a single disease, termed IgG4RD. Recently revised diagnostic criteria for IgG4-RD include 1) clinical or imaging findings So Hyun Yim Jae Seob Yoon Chang Hun Lee Jiyoung Kim","PeriodicalId":324902,"journal":{"name":"Journal of Clinical Neurology (Seoul, Korea)","volume":" ","pages":"481-483"},"PeriodicalIF":0.0000,"publicationDate":"2022-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5c/1b/jcn-18-481.PMC9262458.pdf","citationCount":"0","resultStr":"{\"title\":\"Hypertrophic Pachymeningitis and Interstitial Lung Disease in IgG4-Related Disease.\",\"authors\":\"So Hyun Yim, Jae Seob Yoon, Chang Hun Lee, Jiyoung Kim\",\"doi\":\"10.3988/jcn.2022.18.4.481\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Dear Editor, IgG4-related disease (IgG4-RD) is an immune-mediated inflammatory condition characterized by elevated serum IgG4 and affected organs being infiltrated by IgG4-positive plasma cells.1 This disease can affect multiple organs, but rarely involves the central nervous system (CNS).2 Here we report a case of IgG4-RD presenting as hypertrophic pachymeningitis (HP), which was confirmed in a lung biopsy. A 57-year-old female presented to our hospital with a throbbing headache that began 1 year previously. The pain persisted in the entire head and was more severe on the right side; the patient also had interstitial lung disease (ILD) (Fig. 1A). Although the patient did not present with joint tenderness, the presence of rheumatoid arthritis was supported by elevated C-reactive protein and an increased erythrocyte sedimentation rate. She had been prescribed methylprednisolone (2 mg/day) and tacrolimus (0.5 mg/day) for rheumatoid arthritis. Brain magnetic resonance imaging (MRI) performed in another hospital 5 months previously did not detect any structural lesions that could explain the headache symptoms (Fig. 1B). The patient had been diagnosed with chronic migraine at that time. Despite taking both acute and preventive migraine medications for 5 months, the headache became more severe and interfered with her daily physical activities and the quality of sleep at nighttime. Brain MRI performed upon admission to our hospital revealed pachymeningeal thickening with enhancement in the right hemisphere (Fig. 1C), which had not been found in the previous MRI. An examination of the CSF revealed slight elevation of the WBC count (12/μL, lymphocyte-dominant), whereas protein (37.2 mg/dL) and glucose (66.0 mg/dL) levels were within the normal ranges. Attributing the headaches to IgG4-RD was considered based on the HP revealed by brain MRI and the ILD comorbidity. We investigated the patient’s serum for subclasses of IgG, and found elevated IgG4 (186.4 mg/dL, reference range: 3.9–86.4 mg/dL). A lung biopsy was performed to confirm the diagnosis, because it is safer and easier than a meningeal biopsy. The lung biopsy revealed obliteration of venular vessels and storiform fibrosis with infiltration by lymphoplasma cells (Fig. 1E and F). IgG and IgG4 were found in plasma cells by immunohistochemistry (Fig. 1G and H). Based on the clinical and radiological features observed and the serological and pathological findings, the patient was diagnosed with IgG4-RD.3 She was treated with a high dose of prednisolone (1,000 mg/day for 5 days), followed by rituximab (375 mg/m2). Subsequent MRI revealed decreased pachymeningeal enhancement (Fig. 1D). IgG4-RD can affect various organs, and in this case two organs were involved: the lungs and the brain. The most commonly affected body parts include the pancreas, salivary and lacrimal glands, biliary tract, thyroid, kidney, and lung, while the CNS is rarely involved.4 Diseases that can affect each of these organs are type 1 autoimmune pancreatitis, Mikulicz disease, IgGrelated sclerosing cholangitis, and Riedel’s thyroiditis, and their common clinical, laboratory, and histological features have led to them being classified into a single disease, termed IgG4RD. Recently revised diagnostic criteria for IgG4-RD include 1) clinical or imaging findings So Hyun Yim Jae Seob Yoon Chang Hun Lee Jiyoung Kim\",\"PeriodicalId\":324902,\"journal\":{\"name\":\"Journal of Clinical Neurology (Seoul, Korea)\",\"volume\":\" \",\"pages\":\"481-483\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5c/1b/jcn-18-481.PMC9262458.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Neurology (Seoul, Korea)\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3988/jcn.2022.18.4.481\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Neurology (Seoul, Korea)","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3988/jcn.2022.18.4.481","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Hypertrophic Pachymeningitis and Interstitial Lung Disease in IgG4-Related Disease.
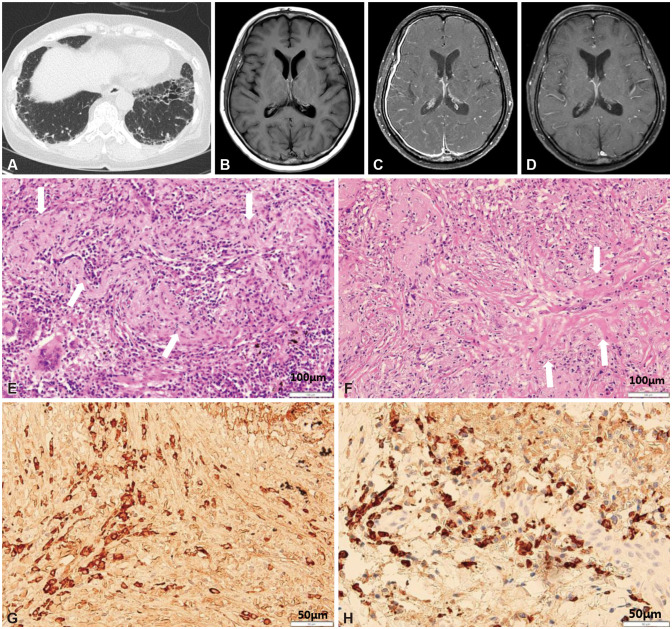
Dear Editor, IgG4-related disease (IgG4-RD) is an immune-mediated inflammatory condition characterized by elevated serum IgG4 and affected organs being infiltrated by IgG4-positive plasma cells.1 This disease can affect multiple organs, but rarely involves the central nervous system (CNS).2 Here we report a case of IgG4-RD presenting as hypertrophic pachymeningitis (HP), which was confirmed in a lung biopsy. A 57-year-old female presented to our hospital with a throbbing headache that began 1 year previously. The pain persisted in the entire head and was more severe on the right side; the patient also had interstitial lung disease (ILD) (Fig. 1A). Although the patient did not present with joint tenderness, the presence of rheumatoid arthritis was supported by elevated C-reactive protein and an increased erythrocyte sedimentation rate. She had been prescribed methylprednisolone (2 mg/day) and tacrolimus (0.5 mg/day) for rheumatoid arthritis. Brain magnetic resonance imaging (MRI) performed in another hospital 5 months previously did not detect any structural lesions that could explain the headache symptoms (Fig. 1B). The patient had been diagnosed with chronic migraine at that time. Despite taking both acute and preventive migraine medications for 5 months, the headache became more severe and interfered with her daily physical activities and the quality of sleep at nighttime. Brain MRI performed upon admission to our hospital revealed pachymeningeal thickening with enhancement in the right hemisphere (Fig. 1C), which had not been found in the previous MRI. An examination of the CSF revealed slight elevation of the WBC count (12/μL, lymphocyte-dominant), whereas protein (37.2 mg/dL) and glucose (66.0 mg/dL) levels were within the normal ranges. Attributing the headaches to IgG4-RD was considered based on the HP revealed by brain MRI and the ILD comorbidity. We investigated the patient’s serum for subclasses of IgG, and found elevated IgG4 (186.4 mg/dL, reference range: 3.9–86.4 mg/dL). A lung biopsy was performed to confirm the diagnosis, because it is safer and easier than a meningeal biopsy. The lung biopsy revealed obliteration of venular vessels and storiform fibrosis with infiltration by lymphoplasma cells (Fig. 1E and F). IgG and IgG4 were found in plasma cells by immunohistochemistry (Fig. 1G and H). Based on the clinical and radiological features observed and the serological and pathological findings, the patient was diagnosed with IgG4-RD.3 She was treated with a high dose of prednisolone (1,000 mg/day for 5 days), followed by rituximab (375 mg/m2). Subsequent MRI revealed decreased pachymeningeal enhancement (Fig. 1D). IgG4-RD can affect various organs, and in this case two organs were involved: the lungs and the brain. The most commonly affected body parts include the pancreas, salivary and lacrimal glands, biliary tract, thyroid, kidney, and lung, while the CNS is rarely involved.4 Diseases that can affect each of these organs are type 1 autoimmune pancreatitis, Mikulicz disease, IgGrelated sclerosing cholangitis, and Riedel’s thyroiditis, and their common clinical, laboratory, and histological features have led to them being classified into a single disease, termed IgG4RD. Recently revised diagnostic criteria for IgG4-RD include 1) clinical or imaging findings So Hyun Yim Jae Seob Yoon Chang Hun Lee Jiyoung Kim

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


