{"title":"南非三级儿科重症监护室拔管失败的危险因素和结果。","authors":"M-C F Kilba, S Salie, B M Morrow","doi":"10.7196/SAJCC.2022.v38i1.513","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Extubation failure contributes to poor outcome of mechanically ventilated children, yet the prevalence and risk factors have been poorly studied in South African (SA) children.</p><p><strong>Objectives: </strong>To determine the prevalence, risk factors and outcomes of extubation failure in an SA paediatric intensive care unit (PICU).</p><p><strong>Methods: </strong>This was a prospective, observational study of all mechanically ventilated children admitted to a tertiary PICU in Cape Town, SA. Extubation failure was defined as requiring re-intubation within 48 hours of planned extubation.</p><p><strong>Results: </strong>There were 219 episodes of mechanical ventilation in 204 children (median (interquartile range (IQR)) age 8 (1.6 - 44.4) months). Twenty-one of 184 (11.4%) planned extubations (95% confidence interval (CI) 7.2% - 16.9%) failed. Emergency cardiac admissions (adjusted odds ratio (aOR) 7.58 (95% CI 1.90 - 30.29), dysmorphology (aOR 4.90; 95% CI 1.49 - 16.14), prematurity (aOR 4.39; 95% CI 1.24 - 15.57), and ventilation ≥48 hours (aOR 6.42 (95% CI 1.57 - 26.22) were associated with extubation failure. Children who failed extubation had longer durations of ventilation (231 hours (146.0 - 341.0) v. 53 hours (21.7 - 123.0); p<0.0001); longer duration of PICU (15 (9 - 20) days v. 5 (2 - 9) days; p<0.0001) and hospital length of stay (32 (21 - 53) days v. 15 (8 - 27) days; p=0.009); and higher 30-day mortality (28.6% v. 6.7%; p=0.001) than successfully extubated children.</p><p><strong>Conclusion: </strong>Extubation failure was associated with significant morbidity and mortality in our setting. Risk factors for extubation failure identified in our context were similar to those reported in other settings.</p><p><strong>Contributions of the study: </strong>This study provides novel data on the prevalence, risk factors and outcomes associated with extubation failure in a single-centre South African PICU. The results of this study may help identify high-risk groups for extubation failure within our local context, and forms a basis for practice improvement initiatives aimed at decreasing extubation failure rates and improving outcomes.</p>","PeriodicalId":75194,"journal":{"name":"The Southern African journal of critical care : the official journal of the Critical Care Society","volume":" ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2022-05-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ed/ca/SAJCC-38-1-513.PMC9233282.pdf","citationCount":"1","resultStr":"{\"title\":\"Risk factors and outcomes of extubation failure in a South African tertiary paediatric intensive care unit.\",\"authors\":\"M-C F Kilba, S Salie, B M Morrow\",\"doi\":\"10.7196/SAJCC.2022.v38i1.513\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Extubation failure contributes to poor outcome of mechanically ventilated children, yet the prevalence and risk factors have been poorly studied in South African (SA) children.</p><p><strong>Objectives: </strong>To determine the prevalence, risk factors and outcomes of extubation failure in an SA paediatric intensive care unit (PICU).</p><p><strong>Methods: </strong>This was a prospective, observational study of all mechanically ventilated children admitted to a tertiary PICU in Cape Town, SA. Extubation failure was defined as requiring re-intubation within 48 hours of planned extubation.</p><p><strong>Results: </strong>There were 219 episodes of mechanical ventilation in 204 children (median (interquartile range (IQR)) age 8 (1.6 - 44.4) months). Twenty-one of 184 (11.4%) planned extubations (95% confidence interval (CI) 7.2% - 16.9%) failed. Emergency cardiac admissions (adjusted odds ratio (aOR) 7.58 (95% CI 1.90 - 30.29), dysmorphology (aOR 4.90; 95% CI 1.49 - 16.14), prematurity (aOR 4.39; 95% CI 1.24 - 15.57), and ventilation ≥48 hours (aOR 6.42 (95% CI 1.57 - 26.22) were associated with extubation failure. Children who failed extubation had longer durations of ventilation (231 hours (146.0 - 341.0) v. 53 hours (21.7 - 123.0); p<0.0001); longer duration of PICU (15 (9 - 20) days v. 5 (2 - 9) days; p<0.0001) and hospital length of stay (32 (21 - 53) days v. 15 (8 - 27) days; p=0.009); and higher 30-day mortality (28.6% v. 6.7%; p=0.001) than successfully extubated children.</p><p><strong>Conclusion: </strong>Extubation failure was associated with significant morbidity and mortality in our setting. Risk factors for extubation failure identified in our context were similar to those reported in other settings.</p><p><strong>Contributions of the study: </strong>This study provides novel data on the prevalence, risk factors and outcomes associated with extubation failure in a single-centre South African PICU. The results of this study may help identify high-risk groups for extubation failure within our local context, and forms a basis for practice improvement initiatives aimed at decreasing extubation failure rates and improving outcomes.</p>\",\"PeriodicalId\":75194,\"journal\":{\"name\":\"The Southern African journal of critical care : the official journal of the Critical Care Society\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-05-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ed/ca/SAJCC-38-1-513.PMC9233282.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Southern African journal of critical care : the official journal of the Critical Care Society\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.7196/SAJCC.2022.v38i1.513\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Southern African journal of critical care : the official journal of the Critical Care Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7196/SAJCC.2022.v38i1.513","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
摘要
背景:拔管失败导致机械通气儿童预后不良,但其在南非儿童中的患病率和危险因素研究甚少。目的:确定SA儿科重症监护病房(PICU)拔管失败的患病率、危险因素和结局。方法:这是一项前瞻性观察性研究,纳入南非开普敦第三重症监护病房所有机械通气儿童。拔管失败定义为在计划拔管48小时内需要重新插管。结果:204例患儿(中位(四分位间距(IQR))年龄为8(1.6 - 44.4)个月)219次机械通气。184例计划拔管中有21例(11.4%)失败(95%置信区间(CI) 7.2% - 16.9%)。急诊心脏入院(调整优势比(aOR) 7.58 (95% CI 1.90 - 30.29),畸形(aOR 4.90;95% CI 1.49 - 16.14),早产(aOR 4.39;95% CI 1.24 - 15.57),通气≥48小时(aOR 6.42 (95% CI 1.57 - 26.22)与拔管失败相关。拔管失败的患儿通气时间较长(231小时(146.0 - 341.0)vs . 53小时(21.7 - 123.0);结论:拔管失败与本研究中显著的发病率和死亡率相关。在我们的研究中发现的拔管失败的危险因素与其他研究中报道的相似。研究贡献:本研究提供了与单中心南非PICU拔管失败相关的患病率、风险因素和结果的新数据。本研究的结果可能有助于确定我们当地拔管失败的高危人群,并形成旨在降低拔管失败率和改善结果的实践改进倡议的基础。
Risk factors and outcomes of extubation failure in a South African tertiary paediatric intensive care unit.
Background: Extubation failure contributes to poor outcome of mechanically ventilated children, yet the prevalence and risk factors have been poorly studied in South African (SA) children.
Objectives: To determine the prevalence, risk factors and outcomes of extubation failure in an SA paediatric intensive care unit (PICU).
Methods: This was a prospective, observational study of all mechanically ventilated children admitted to a tertiary PICU in Cape Town, SA. Extubation failure was defined as requiring re-intubation within 48 hours of planned extubation.
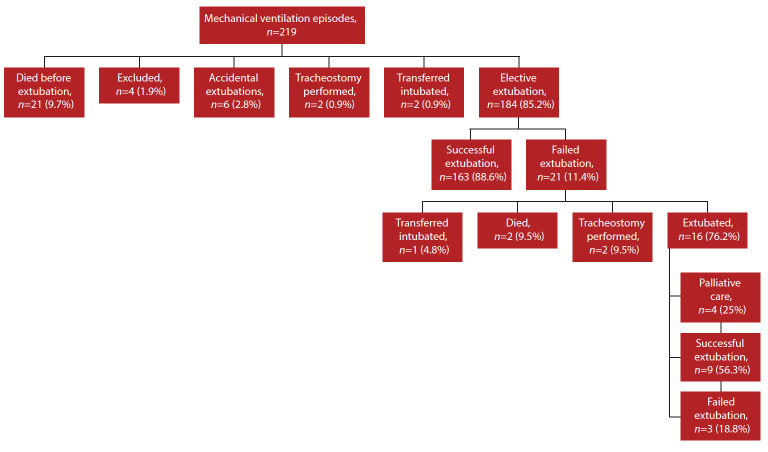
Results: There were 219 episodes of mechanical ventilation in 204 children (median (interquartile range (IQR)) age 8 (1.6 - 44.4) months). Twenty-one of 184 (11.4%) planned extubations (95% confidence interval (CI) 7.2% - 16.9%) failed. Emergency cardiac admissions (adjusted odds ratio (aOR) 7.58 (95% CI 1.90 - 30.29), dysmorphology (aOR 4.90; 95% CI 1.49 - 16.14), prematurity (aOR 4.39; 95% CI 1.24 - 15.57), and ventilation ≥48 hours (aOR 6.42 (95% CI 1.57 - 26.22) were associated with extubation failure. Children who failed extubation had longer durations of ventilation (231 hours (146.0 - 341.0) v. 53 hours (21.7 - 123.0); p<0.0001); longer duration of PICU (15 (9 - 20) days v. 5 (2 - 9) days; p<0.0001) and hospital length of stay (32 (21 - 53) days v. 15 (8 - 27) days; p=0.009); and higher 30-day mortality (28.6% v. 6.7%; p=0.001) than successfully extubated children.
Conclusion: Extubation failure was associated with significant morbidity and mortality in our setting. Risk factors for extubation failure identified in our context were similar to those reported in other settings.
Contributions of the study: This study provides novel data on the prevalence, risk factors and outcomes associated with extubation failure in a single-centre South African PICU. The results of this study may help identify high-risk groups for extubation failure within our local context, and forms a basis for practice improvement initiatives aimed at decreasing extubation failure rates and improving outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


