Steven H Lin, Kaiping Liao, Xiudong Lei, Vivek Verma, Sherif Shaaban, Percy Lee, Aileen B Chen, Albert C Koong, Wayne L Hoftstetter, Steven J Frank, Zhongxing Liao, Ya-Chen Tina Shih, Sharon H Giordano, Grace L Smith
{"title":"食管癌质子与光子放射治疗的保健资源利用。","authors":"Steven H Lin, Kaiping Liao, Xiudong Lei, Vivek Verma, Sherif Shaaban, Percy Lee, Aileen B Chen, Albert C Koong, Wayne L Hoftstetter, Steven J Frank, Zhongxing Liao, Ya-Chen Tina Shih, Sharon H Giordano, Grace L Smith","doi":"10.14338/IJPT-22-00001.1","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>In patients treated with chemoradiation for esophageal cancer (EC), randomized trial data demonstrate that proton beam therapy (PBT) reduces toxicities and postoperative complications (POCs) compared with intensity-modulated radiation therapy (IMRT). However, whether radiation therapy modality affects postoperative health care resource utilization remains unknown.</p><p><strong>Materials and methods: </strong>We examined 287 patients with EC who received chemoradiation (prescribed 50.4 Gy/GyE) followed by esophagectomy, including a real-world observational cohort of 237 consecutive patients treated from 2007 to 2013 with PBT (n = 81) versus IMRT (n = 156); and an independent, contemporary comparison cohort of 50 patients from a randomized trial treated from 2012 to 2019 with PBT (n = 21) versus IMRT (n = 29). Postoperative complications were abstracted from medical records. Health care charges were obtained from institutional claims and adjusted for inflation (2021 dollars). Charge differences (Δ = $PBT - $IMRT) were compared by treatment using adjusted generalized linear models with the gamma distribution.</p><p><strong>Results: </strong>Baseline PBT versus IMRT characteristics were not significantly different. In the observational cohort, during the neoadjuvant chemoradiation phase, health care charges were higher for PBT versus IMRT (Δ = +$71,959; 95% confidence interval [CI], $62,274-$82,138; <i>P</i> < .001). There was no difference in surgical charges (Δ = -$2234; 95% CI, -$6003 to $1695; <i>P</i> = .26). However, during postoperative hospitalization following esophagectomy, health care charges were lower for PBT versus IMRT (Δ = -$25,115; 95% CI, -$37,625 to -$9776; <i>P</i> = .003). In the comparison cohort, findings were analogous: Charges were higher for PBT versus IMRT during chemoradiation (Δ = +$61,818; 95% CI, $49,435-$75,069; <i>P</i> < .001), not different for surgery (Δ = -$4784; 95% CI, -$6439 to $3487; <i>P</i> = .25), and lower for PBT postoperatively (Δ = -$27,048; 95% CI, -$41,974 to -$5300; <i>P</i> = .02). Lower postoperative charges for PBT were especially seen among patients with any POCs in the contemporary comparison (Δ = -$176,448; 95% CI, -$209,782 to -$78,813; <i>P</i> = .02).</p><p><strong>Conclusion: </strong>Higher up-front chemoradiation resource utilization for PBT in patients with EC was partially offset postoperatively, moderated by reduction in POC risks. Results extend existing clinical evidence of toxicity reduction with PBT.</p>","PeriodicalId":36923,"journal":{"name":"International Journal of Particle Therapy","volume":"9 1","pages":"18-27"},"PeriodicalIF":2.0000,"publicationDate":"2022-06-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9238132/pdf/","citationCount":"2","resultStr":"{\"title\":\"Health Care Resource Utilization for Esophageal Cancer Using Proton versus Photon Radiation Therapy.\",\"authors\":\"Steven H Lin, Kaiping Liao, Xiudong Lei, Vivek Verma, Sherif Shaaban, Percy Lee, Aileen B Chen, Albert C Koong, Wayne L Hoftstetter, Steven J Frank, Zhongxing Liao, Ya-Chen Tina Shih, Sharon H Giordano, Grace L Smith\",\"doi\":\"10.14338/IJPT-22-00001.1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>In patients treated with chemoradiation for esophageal cancer (EC), randomized trial data demonstrate that proton beam therapy (PBT) reduces toxicities and postoperative complications (POCs) compared with intensity-modulated radiation therapy (IMRT). However, whether radiation therapy modality affects postoperative health care resource utilization remains unknown.</p><p><strong>Materials and methods: </strong>We examined 287 patients with EC who received chemoradiation (prescribed 50.4 Gy/GyE) followed by esophagectomy, including a real-world observational cohort of 237 consecutive patients treated from 2007 to 2013 with PBT (n = 81) versus IMRT (n = 156); and an independent, contemporary comparison cohort of 50 patients from a randomized trial treated from 2012 to 2019 with PBT (n = 21) versus IMRT (n = 29). Postoperative complications were abstracted from medical records. Health care charges were obtained from institutional claims and adjusted for inflation (2021 dollars). Charge differences (Δ = $PBT - $IMRT) were compared by treatment using adjusted generalized linear models with the gamma distribution.</p><p><strong>Results: </strong>Baseline PBT versus IMRT characteristics were not significantly different. In the observational cohort, during the neoadjuvant chemoradiation phase, health care charges were higher for PBT versus IMRT (Δ = +$71,959; 95% confidence interval [CI], $62,274-$82,138; <i>P</i> < .001). There was no difference in surgical charges (Δ = -$2234; 95% CI, -$6003 to $1695; <i>P</i> = .26). However, during postoperative hospitalization following esophagectomy, health care charges were lower for PBT versus IMRT (Δ = -$25,115; 95% CI, -$37,625 to -$9776; <i>P</i> = .003). In the comparison cohort, findings were analogous: Charges were higher for PBT versus IMRT during chemoradiation (Δ = +$61,818; 95% CI, $49,435-$75,069; <i>P</i> < .001), not different for surgery (Δ = -$4784; 95% CI, -$6439 to $3487; <i>P</i> = .25), and lower for PBT postoperatively (Δ = -$27,048; 95% CI, -$41,974 to -$5300; <i>P</i> = .02). Lower postoperative charges for PBT were especially seen among patients with any POCs in the contemporary comparison (Δ = -$176,448; 95% CI, -$209,782 to -$78,813; <i>P</i> = .02).</p><p><strong>Conclusion: </strong>Higher up-front chemoradiation resource utilization for PBT in patients with EC was partially offset postoperatively, moderated by reduction in POC risks. Results extend existing clinical evidence of toxicity reduction with PBT.</p>\",\"PeriodicalId\":36923,\"journal\":{\"name\":\"International Journal of Particle Therapy\",\"volume\":\"9 1\",\"pages\":\"18-27\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2022-06-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9238132/pdf/\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Particle Therapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14338/IJPT-22-00001.1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Particle Therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14338/IJPT-22-00001.1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
Health Care Resource Utilization for Esophageal Cancer Using Proton versus Photon Radiation Therapy.
Purpose: In patients treated with chemoradiation for esophageal cancer (EC), randomized trial data demonstrate that proton beam therapy (PBT) reduces toxicities and postoperative complications (POCs) compared with intensity-modulated radiation therapy (IMRT). However, whether radiation therapy modality affects postoperative health care resource utilization remains unknown.
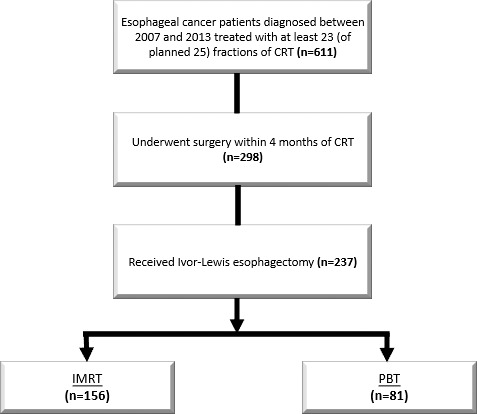
Materials and methods: We examined 287 patients with EC who received chemoradiation (prescribed 50.4 Gy/GyE) followed by esophagectomy, including a real-world observational cohort of 237 consecutive patients treated from 2007 to 2013 with PBT (n = 81) versus IMRT (n = 156); and an independent, contemporary comparison cohort of 50 patients from a randomized trial treated from 2012 to 2019 with PBT (n = 21) versus IMRT (n = 29). Postoperative complications were abstracted from medical records. Health care charges were obtained from institutional claims and adjusted for inflation (2021 dollars). Charge differences (Δ = $PBT - $IMRT) were compared by treatment using adjusted generalized linear models with the gamma distribution.
Results: Baseline PBT versus IMRT characteristics were not significantly different. In the observational cohort, during the neoadjuvant chemoradiation phase, health care charges were higher for PBT versus IMRT (Δ = +$71,959; 95% confidence interval [CI], $62,274-$82,138; P < .001). There was no difference in surgical charges (Δ = -$2234; 95% CI, -$6003 to $1695; P = .26). However, during postoperative hospitalization following esophagectomy, health care charges were lower for PBT versus IMRT (Δ = -$25,115; 95% CI, -$37,625 to -$9776; P = .003). In the comparison cohort, findings were analogous: Charges were higher for PBT versus IMRT during chemoradiation (Δ = +$61,818; 95% CI, $49,435-$75,069; P < .001), not different for surgery (Δ = -$4784; 95% CI, -$6439 to $3487; P = .25), and lower for PBT postoperatively (Δ = -$27,048; 95% CI, -$41,974 to -$5300; P = .02). Lower postoperative charges for PBT were especially seen among patients with any POCs in the contemporary comparison (Δ = -$176,448; 95% CI, -$209,782 to -$78,813; P = .02).
Conclusion: Higher up-front chemoradiation resource utilization for PBT in patients with EC was partially offset postoperatively, moderated by reduction in POC risks. Results extend existing clinical evidence of toxicity reduction with PBT.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


