Nóra Suszták, István Besznyák, Kálmán Almási, Attila Bursics, Dóra Kelemen, David W Borowski, Balázs Bánky
{"title":"体外动脉亚甲基蓝浸润提高结直肠癌淋巴结分期准确性和长期生存益处。","authors":"Nóra Suszták, István Besznyák, Kálmán Almási, Attila Bursics, Dóra Kelemen, David W Borowski, Balázs Bánky","doi":"10.3389/pore.2022.1610742","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction:</b> <i>Ex vivo</i> methylene blue (MB) injection into the main supplying arteries of the colorectal specimen after surgical removal is an uncomplicated technique to support lymph node harvest during pathological evaluation. The primary aim of this randomized, interventional, bicentric trial was to evaluate the impact of MB injection on lymph node yield, with secondary aims assessing the accuracy of lymph node staging and the effect on 5-year overall survival for patients undergoing resection of colorectal cancer. <b>Methods:</b> In the study period between December 2013 and August 2015, 200 colorectal resections were performed at two independent onco-surgery centers of Hungary. Following surgical resection, each specimen was randomly assigned either to the control (standard pathological work-up) or to the MB staining group before formaldehyde fixation. Patient-level surgical and clinical data were retrieved from routinely collected clinical datasets. Survival status data were obtained from the National Health Insurance Fund of Hungary. <b>Results:</b> A total of 162 specimens, 82 in the control and 80 in the MB groups, were included for analysis. Baseline characteristics were equally distributed among study groups, except for specimen length. Both the median of total number of lymph nodes retrieved (control 11 ± 8 [0-33] nodes vs. MB 14 ± 6 [0-42] nodes; <i>p</i> < 0.01), and the ratio of cases with at least 12 removed lymph nodes (36/82, 43.9% vs. 53/80, 66.3%; <i>p</i> < 0.01) were higher in the MB group. The rate of accurate lymph node staging was non-significantly improved. As for rectal cancer, nodal staging accuracy (16/31, 51.6% vs. 23/30, 76.7%; <i>p</i> = 0.04) and the proportion with minimum 12 lymph node retrieval (7/31, 22.6%, vs. 18/30, 60%; <i>p</i> < 0.01) was improved by MB injection. In Mantel-Cox regression, a statistically significant survival benefit with methylene blue injection at 5 years post-surgery was proven (51.2% vs. 68.8%; <i>p</i> = 0.04). <b>Conclusion:</b> In our experience, postoperative <i>ex vivo</i> arterial methylene blue injection appears to be an uncomplicated technique, improving lymph node yield and decreasing the chance of insufficient nodal staging. The technique might also associate with a 5-year overall survival benefit.</p>","PeriodicalId":411887,"journal":{"name":"Pathology oncology research : POR","volume":" ","pages":"1610742"},"PeriodicalIF":0.0000,"publicationDate":"2022-10-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9624224/pdf/","citationCount":"0","resultStr":"{\"title\":\"Improved Accuracy of Lymph Node Staging and Long-Term Survival Benefit in Colorectal Cancer With <i>Ex Vivo</i> Arterial Methylene Blue Infiltration.\",\"authors\":\"Nóra Suszták, István Besznyák, Kálmán Almási, Attila Bursics, Dóra Kelemen, David W Borowski, Balázs Bánky\",\"doi\":\"10.3389/pore.2022.1610742\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Introduction:</b> <i>Ex vivo</i> methylene blue (MB) injection into the main supplying arteries of the colorectal specimen after surgical removal is an uncomplicated technique to support lymph node harvest during pathological evaluation. The primary aim of this randomized, interventional, bicentric trial was to evaluate the impact of MB injection on lymph node yield, with secondary aims assessing the accuracy of lymph node staging and the effect on 5-year overall survival for patients undergoing resection of colorectal cancer. <b>Methods:</b> In the study period between December 2013 and August 2015, 200 colorectal resections were performed at two independent onco-surgery centers of Hungary. Following surgical resection, each specimen was randomly assigned either to the control (standard pathological work-up) or to the MB staining group before formaldehyde fixation. Patient-level surgical and clinical data were retrieved from routinely collected clinical datasets. Survival status data were obtained from the National Health Insurance Fund of Hungary. <b>Results:</b> A total of 162 specimens, 82 in the control and 80 in the MB groups, were included for analysis. Baseline characteristics were equally distributed among study groups, except for specimen length. Both the median of total number of lymph nodes retrieved (control 11 ± 8 [0-33] nodes vs. MB 14 ± 6 [0-42] nodes; <i>p</i> < 0.01), and the ratio of cases with at least 12 removed lymph nodes (36/82, 43.9% vs. 53/80, 66.3%; <i>p</i> < 0.01) were higher in the MB group. The rate of accurate lymph node staging was non-significantly improved. As for rectal cancer, nodal staging accuracy (16/31, 51.6% vs. 23/30, 76.7%; <i>p</i> = 0.04) and the proportion with minimum 12 lymph node retrieval (7/31, 22.6%, vs. 18/30, 60%; <i>p</i> < 0.01) was improved by MB injection. In Mantel-Cox regression, a statistically significant survival benefit with methylene blue injection at 5 years post-surgery was proven (51.2% vs. 68.8%; <i>p</i> = 0.04). <b>Conclusion:</b> In our experience, postoperative <i>ex vivo</i> arterial methylene blue injection appears to be an uncomplicated technique, improving lymph node yield and decreasing the chance of insufficient nodal staging. The technique might also associate with a 5-year overall survival benefit.</p>\",\"PeriodicalId\":411887,\"journal\":{\"name\":\"Pathology oncology research : POR\",\"volume\":\" \",\"pages\":\"1610742\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-10-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9624224/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pathology oncology research : POR\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3389/pore.2022.1610742\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pathology oncology research : POR","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/pore.2022.1610742","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
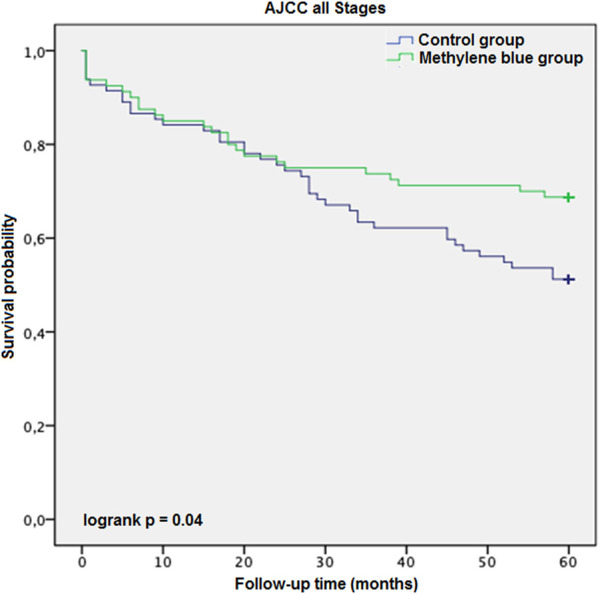
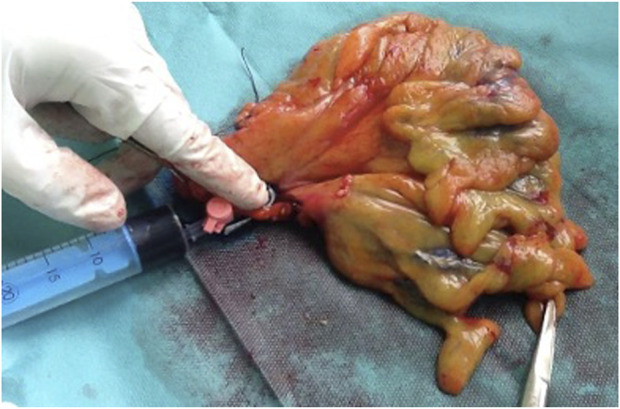
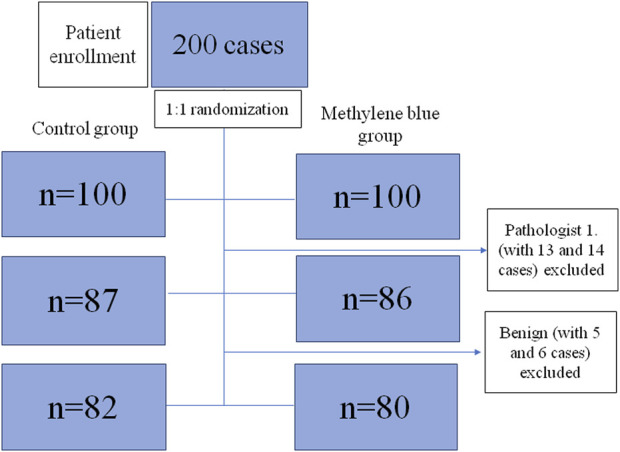
在结直肠标本手术切除后,体外亚甲基蓝(MB)注射到主要供应动脉是一种简单的技术,可以在病理评估期间支持淋巴结采集。这项随机、介入性、双中心试验的主要目的是评估MB注射对淋巴结生成量的影响,次要目的是评估淋巴结分期的准确性以及对结直肠癌切除术患者5年总生存率的影响。方法:2013年12月至2015年8月,在匈牙利两家独立的肿瘤外科中心进行200例结直肠切除术。手术切除后,每个标本被随机分配到对照组(标准病理检查)或甲醛固定前MB染色组。从常规收集的临床数据集中检索患者水平的手术和临床数据。生存状况数据来自匈牙利国家健康保险基金。结果:共纳入162例标本进行分析,其中对照组82例,MB组80例。除标本长度外,各组基线特征分布均匀。淋巴结总数中位数(对照组11±8[0-33]个淋巴结vs. MB 14±6[0-42]个淋巴结;P < 0.01),且至少有12个淋巴结被切除的比例(36/ 82,43.9% vs. 53/ 80,66.3%;p < 0.01), MB组较高。准确的淋巴结分期率无明显提高。直肠癌的分期准确率(16/31,51.6% vs. 23/30, 76.7%;P = 0.04),最小12个淋巴结切除的比例(7/31,22.6%,比18/30,60%;p < 0.01)。在Mantel-Cox回归中,亚甲蓝注射在术后5年的生存获益被证明具有统计学意义(51.2% vs 68.8%;P = 0.04)。结论:根据我们的经验,术后体外动脉注射亚甲基蓝似乎是一种简单的技术,可以提高淋巴结产量,减少淋巴结分期不足的机会。这项技术也可能与5年总体生存获益有关。
Improved Accuracy of Lymph Node Staging and Long-Term Survival Benefit in Colorectal Cancer With Ex Vivo Arterial Methylene Blue Infiltration.
Introduction:Ex vivo methylene blue (MB) injection into the main supplying arteries of the colorectal specimen after surgical removal is an uncomplicated technique to support lymph node harvest during pathological evaluation. The primary aim of this randomized, interventional, bicentric trial was to evaluate the impact of MB injection on lymph node yield, with secondary aims assessing the accuracy of lymph node staging and the effect on 5-year overall survival for patients undergoing resection of colorectal cancer. Methods: In the study period between December 2013 and August 2015, 200 colorectal resections were performed at two independent onco-surgery centers of Hungary. Following surgical resection, each specimen was randomly assigned either to the control (standard pathological work-up) or to the MB staining group before formaldehyde fixation. Patient-level surgical and clinical data were retrieved from routinely collected clinical datasets. Survival status data were obtained from the National Health Insurance Fund of Hungary. Results: A total of 162 specimens, 82 in the control and 80 in the MB groups, were included for analysis. Baseline characteristics were equally distributed among study groups, except for specimen length. Both the median of total number of lymph nodes retrieved (control 11 ± 8 [0-33] nodes vs. MB 14 ± 6 [0-42] nodes; p < 0.01), and the ratio of cases with at least 12 removed lymph nodes (36/82, 43.9% vs. 53/80, 66.3%; p < 0.01) were higher in the MB group. The rate of accurate lymph node staging was non-significantly improved. As for rectal cancer, nodal staging accuracy (16/31, 51.6% vs. 23/30, 76.7%; p = 0.04) and the proportion with minimum 12 lymph node retrieval (7/31, 22.6%, vs. 18/30, 60%; p < 0.01) was improved by MB injection. In Mantel-Cox regression, a statistically significant survival benefit with methylene blue injection at 5 years post-surgery was proven (51.2% vs. 68.8%; p = 0.04). Conclusion: In our experience, postoperative ex vivo arterial methylene blue injection appears to be an uncomplicated technique, improving lymph node yield and decreasing the chance of insufficient nodal staging. The technique might also associate with a 5-year overall survival benefit.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


