Nada M Abou-Karam, Melissa E Jump, Jingying Jiao, Andrew N Schmelz
{"title":"联邦合格医疗中心的药剂师-医生分开共享访问:从使用远程医疗的新型报销模式中吸取的教训。","authors":"Nada M Abou-Karam, Melissa E Jump, Jingying Jiao, Andrew N Schmelz","doi":"10.24926/iip.v13i1.4451","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction:</b> The Federally Qualified Health Center (FQHC) setting poses unique challenges to reimbursement of services provided by ambulatory care pharmacists; however, recent changes to telemedicine reimbursement have created new opportunities to help overcome these challenges. This article describes the experience and outcomes of the implementation of a novel, pharmacist-physician split-shared telehealth model at AltaMed Medical Group, a large, multi-site FQHC in Los Angeles and Orange counties. <b>Program Development and Implementation</b>: A pilot program for pharmacist-physician split shared tele-visits was launched at one clinic site with one clinical pharmacist and has since been expanded to a total of 6 sites and 5 clinical pharmacists. Prior to this program, clinical pharmacists saw patients for diabetes mellitus (DM) video-conference disease management appointments. With the launch of the pilot program, additional steps were added to pre-existing workflows to create a model in which visits with the clinical pharmacists were followed by an \"enhanced visit\" with an eligible, billable clinic provider. <b>Outcomes</b>: Average A1c change for all patients in the split-shared model was -1.5%, and average A1c change for program graduates from enrollment through graduation was -3.8%. Evidence from similar services have also been associated with significant increases in revenue from a split-shared model, indicating this design can be a viable option for financial justification of ambulatory care pharmacy services. <b>Conclusion:</b> In the setting of current limitations, we advocate for increased utilization of shared visits and split-shared visits as a viable method to generate revenue and aid in the justification of clinical pharmacy services.</p>","PeriodicalId":13646,"journal":{"name":"Innovations in Pharmacy","volume":" ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2022-04-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/db/f3/21550417-13-01-4451.PMC9598973.pdf","citationCount":"0","resultStr":"{\"title\":\"Pharmacist-Physician Split-Shared Visits in a Federally Qualified Health Center: Lessons Learned from a Novel Reimbursement Model using Telehealth.\",\"authors\":\"Nada M Abou-Karam, Melissa E Jump, Jingying Jiao, Andrew N Schmelz\",\"doi\":\"10.24926/iip.v13i1.4451\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Introduction:</b> The Federally Qualified Health Center (FQHC) setting poses unique challenges to reimbursement of services provided by ambulatory care pharmacists; however, recent changes to telemedicine reimbursement have created new opportunities to help overcome these challenges. This article describes the experience and outcomes of the implementation of a novel, pharmacist-physician split-shared telehealth model at AltaMed Medical Group, a large, multi-site FQHC in Los Angeles and Orange counties. <b>Program Development and Implementation</b>: A pilot program for pharmacist-physician split shared tele-visits was launched at one clinic site with one clinical pharmacist and has since been expanded to a total of 6 sites and 5 clinical pharmacists. Prior to this program, clinical pharmacists saw patients for diabetes mellitus (DM) video-conference disease management appointments. With the launch of the pilot program, additional steps were added to pre-existing workflows to create a model in which visits with the clinical pharmacists were followed by an \\\"enhanced visit\\\" with an eligible, billable clinic provider. <b>Outcomes</b>: Average A1c change for all patients in the split-shared model was -1.5%, and average A1c change for program graduates from enrollment through graduation was -3.8%. Evidence from similar services have also been associated with significant increases in revenue from a split-shared model, indicating this design can be a viable option for financial justification of ambulatory care pharmacy services. <b>Conclusion:</b> In the setting of current limitations, we advocate for increased utilization of shared visits and split-shared visits as a viable method to generate revenue and aid in the justification of clinical pharmacy services.</p>\",\"PeriodicalId\":13646,\"journal\":{\"name\":\"Innovations in Pharmacy\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-04-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/db/f3/21550417-13-01-4451.PMC9598973.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Innovations in Pharmacy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.24926/iip.v13i1.4451\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Innovations in Pharmacy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.24926/iip.v13i1.4451","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Pharmacist-Physician Split-Shared Visits in a Federally Qualified Health Center: Lessons Learned from a Novel Reimbursement Model using Telehealth.
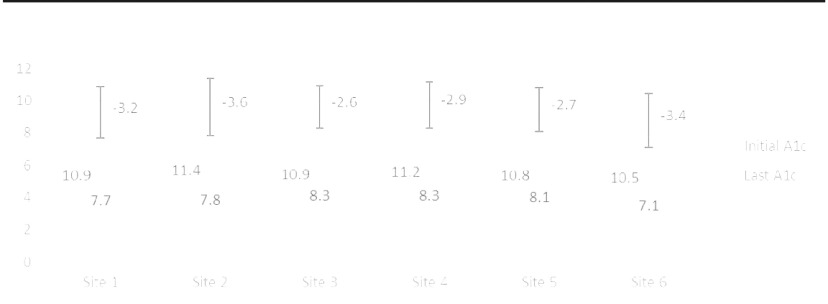
Introduction: The Federally Qualified Health Center (FQHC) setting poses unique challenges to reimbursement of services provided by ambulatory care pharmacists; however, recent changes to telemedicine reimbursement have created new opportunities to help overcome these challenges. This article describes the experience and outcomes of the implementation of a novel, pharmacist-physician split-shared telehealth model at AltaMed Medical Group, a large, multi-site FQHC in Los Angeles and Orange counties. Program Development and Implementation: A pilot program for pharmacist-physician split shared tele-visits was launched at one clinic site with one clinical pharmacist and has since been expanded to a total of 6 sites and 5 clinical pharmacists. Prior to this program, clinical pharmacists saw patients for diabetes mellitus (DM) video-conference disease management appointments. With the launch of the pilot program, additional steps were added to pre-existing workflows to create a model in which visits with the clinical pharmacists were followed by an "enhanced visit" with an eligible, billable clinic provider. Outcomes: Average A1c change for all patients in the split-shared model was -1.5%, and average A1c change for program graduates from enrollment through graduation was -3.8%. Evidence from similar services have also been associated with significant increases in revenue from a split-shared model, indicating this design can be a viable option for financial justification of ambulatory care pharmacy services. Conclusion: In the setting of current limitations, we advocate for increased utilization of shared visits and split-shared visits as a viable method to generate revenue and aid in the justification of clinical pharmacy services.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


