Tao-Ran Yang, Kai Luo, Xiao Deng, Le Xu, Ru-Rong Wang, Peng Ji
{"title":"肌肉减少症在预测急诊剖腹手术术后死亡率中的作用:一项系统回顾和荟萃分析。","authors":"Tao-Ran Yang, Kai Luo, Xiao Deng, Le Xu, Ru-Rong Wang, Peng Ji","doi":"10.1186/s13017-022-00440-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>While emergency laparotomy has been associated with high rates of postoperative mortality and adverse events, preoperative systematic evaluation of patients may improve perioperative outcomes. However, due to the critical condition of the patient and the limited operation time, it is challenging to conduct a comprehensive evaluation. In recent years, sarcopenia is considered a health problem associated with an increased incidence of poor prognosis. This study aimed to investigate the effect of sarcopenia on 30-day mortality and postoperative adverse events in patients undergoing emergency laparotomy.</p><p><strong>Methods: </strong>We systematically searched databases including PubMed, Embase, and Cochrane for all studies comparing emergency laparotomy in patients with and without sarcopenia up to March 1, 2022. The primary outcome was of 30-day postoperative mortality. Secondary outcomes were the length of hospital stay, the incidence of adverse events, number of postoperative intensive care unit (ICU) admissions, and ICU length of stay. Study and outcome-specific risk of bias were assessed using the Quality in Prognosis Studies (QUIPS) tool. We rated the certainty of evidence using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE).</p><p><strong>Result: </strong>A total of 11 eligible studies were included in this study. The results showed that patients with sarcopenia had a higher risk of death 30 days after surgery (OR = 2.42, 95% CI = 1.93-3.05, P < 0.00001). More patients were admitted to ICU after surgery (OR = 1.58, 95% CI = 1.11-2.25, P = 0.01). Both the ICU length of stay (MD = 0.55, 95% CI = 0.05-1.06, P = 0.03) and hospital length of stay (MD = 2.33, 95% CI = 1.33-3.32, P < 0.00001) were longer in the sarcopenia group. The incidence of postoperative complications was also significantly higher in patients with sarcopenia (OR = 1.78, 95% CI = 1.41-2.26, P < 0.00001).</p><p><strong>Conclusion: </strong>In emergency laparotomy, sarcopenia was associated with increased 30-day postoperative mortality. Both the lengths of stay in the ICU and the total length of hospital stay were significantly higher than those in non-sarcopenic patients. Therefore, we concluded that sarcopenia can be used as a tool to identify preoperative high-risk patients, which can be considered to develop new postoperative risk prediction models. Registration number Registered on Prospero with the registration number of CRD42022300132.</p>","PeriodicalId":290899,"journal":{"name":"World Journal of Emergency Surgery : WJES","volume":" ","pages":"36"},"PeriodicalIF":0.0000,"publicationDate":"2022-06-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9233792/pdf/","citationCount":"11","resultStr":"{\"title\":\"Effect of sarcopenia in predicting postoperative mortality in emergency laparotomy: a systematic review and meta-analysis.\",\"authors\":\"Tao-Ran Yang, Kai Luo, Xiao Deng, Le Xu, Ru-Rong Wang, Peng Ji\",\"doi\":\"10.1186/s13017-022-00440-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>While emergency laparotomy has been associated with high rates of postoperative mortality and adverse events, preoperative systematic evaluation of patients may improve perioperative outcomes. However, due to the critical condition of the patient and the limited operation time, it is challenging to conduct a comprehensive evaluation. In recent years, sarcopenia is considered a health problem associated with an increased incidence of poor prognosis. This study aimed to investigate the effect of sarcopenia on 30-day mortality and postoperative adverse events in patients undergoing emergency laparotomy.</p><p><strong>Methods: </strong>We systematically searched databases including PubMed, Embase, and Cochrane for all studies comparing emergency laparotomy in patients with and without sarcopenia up to March 1, 2022. The primary outcome was of 30-day postoperative mortality. Secondary outcomes were the length of hospital stay, the incidence of adverse events, number of postoperative intensive care unit (ICU) admissions, and ICU length of stay. Study and outcome-specific risk of bias were assessed using the Quality in Prognosis Studies (QUIPS) tool. We rated the certainty of evidence using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE).</p><p><strong>Result: </strong>A total of 11 eligible studies were included in this study. The results showed that patients with sarcopenia had a higher risk of death 30 days after surgery (OR = 2.42, 95% CI = 1.93-3.05, P < 0.00001). More patients were admitted to ICU after surgery (OR = 1.58, 95% CI = 1.11-2.25, P = 0.01). Both the ICU length of stay (MD = 0.55, 95% CI = 0.05-1.06, P = 0.03) and hospital length of stay (MD = 2.33, 95% CI = 1.33-3.32, P < 0.00001) were longer in the sarcopenia group. The incidence of postoperative complications was also significantly higher in patients with sarcopenia (OR = 1.78, 95% CI = 1.41-2.26, P < 0.00001).</p><p><strong>Conclusion: </strong>In emergency laparotomy, sarcopenia was associated with increased 30-day postoperative mortality. Both the lengths of stay in the ICU and the total length of hospital stay were significantly higher than those in non-sarcopenic patients. Therefore, we concluded that sarcopenia can be used as a tool to identify preoperative high-risk patients, which can be considered to develop new postoperative risk prediction models. Registration number Registered on Prospero with the registration number of CRD42022300132.</p>\",\"PeriodicalId\":290899,\"journal\":{\"name\":\"World Journal of Emergency Surgery : WJES\",\"volume\":\" \",\"pages\":\"36\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-06-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9233792/pdf/\",\"citationCount\":\"11\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Emergency Surgery : WJES\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13017-022-00440-0\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Emergency Surgery : WJES","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13017-022-00440-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 11
摘要
背景:虽然急诊剖腹手术与术后高死亡率和不良事件相关,但术前系统评估患者可能会改善围手术期预后。但由于患者病情危重,手术时间有限,很难对其进行全面的评估。近年来,肌肉减少症被认为是一种与预后不良发生率增加相关的健康问题。本研究旨在探讨肌肉减少症对急诊剖腹手术患者30天死亡率和术后不良事件的影响。方法:我们系统地检索PubMed、Embase和Cochrane等数据库,检索截至2022年3月1日,所有比较有和没有肌肉减少症患者急诊剖腹手术的研究。主要终点为术后30天死亡率。次要结局是住院时间、不良事件发生率、术后重症监护病房(ICU)入院次数和ICU住院时间。使用预后研究质量(QUIPS)工具评估研究和结果特异性偏倚风险。我们使用推荐、评估、发展和评价分级(GRADE)对证据的确定性进行评级。结果:本研究共纳入11项符合条件的研究。结果显示,肌少症患者术后30天死亡风险较高(OR = 2.42, 95% CI = 1.93-3.05, P)。结论:急诊剖腹手术中,肌少症与术后30天死亡率升高相关。ICU住院时间和总住院时间均明显高于非肌少症患者。因此,我们认为肌少症可作为识别术前高危患者的工具,可考虑开发新的术后风险预测模型。注册号在普洛斯彼罗注册,注册号为CRD42022300132。
Effect of sarcopenia in predicting postoperative mortality in emergency laparotomy: a systematic review and meta-analysis.
Background: While emergency laparotomy has been associated with high rates of postoperative mortality and adverse events, preoperative systematic evaluation of patients may improve perioperative outcomes. However, due to the critical condition of the patient and the limited operation time, it is challenging to conduct a comprehensive evaluation. In recent years, sarcopenia is considered a health problem associated with an increased incidence of poor prognosis. This study aimed to investigate the effect of sarcopenia on 30-day mortality and postoperative adverse events in patients undergoing emergency laparotomy.
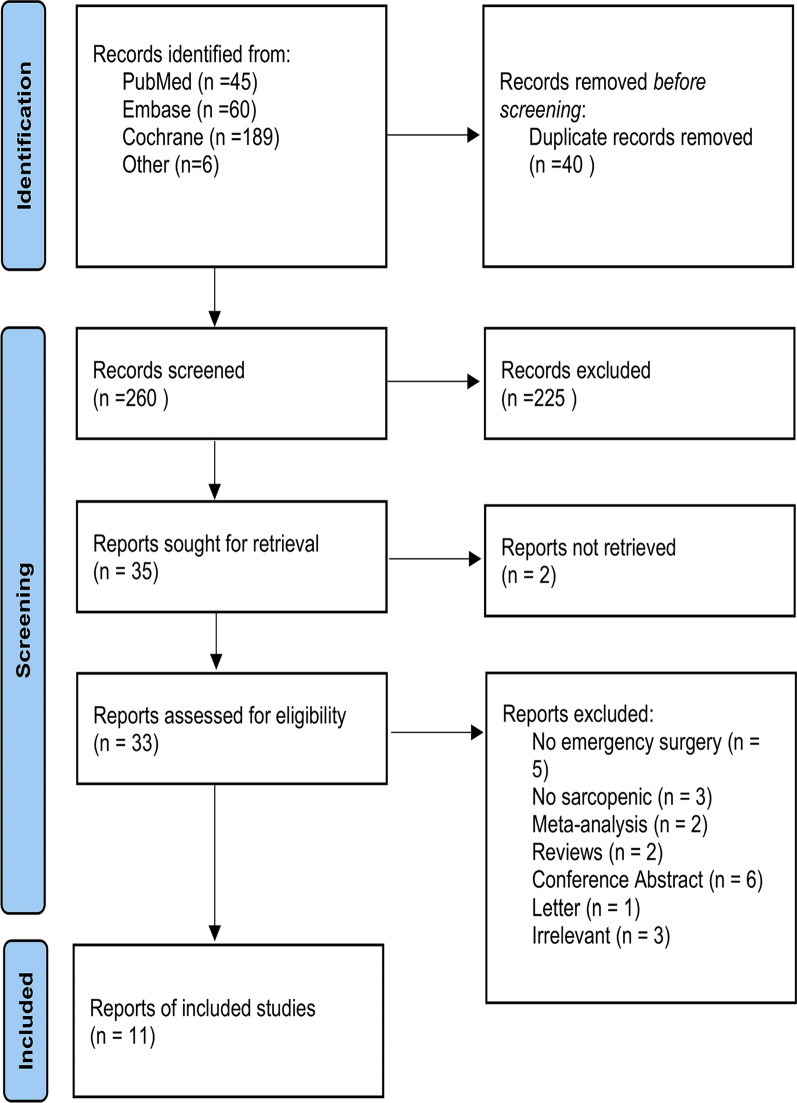
Methods: We systematically searched databases including PubMed, Embase, and Cochrane for all studies comparing emergency laparotomy in patients with and without sarcopenia up to March 1, 2022. The primary outcome was of 30-day postoperative mortality. Secondary outcomes were the length of hospital stay, the incidence of adverse events, number of postoperative intensive care unit (ICU) admissions, and ICU length of stay. Study and outcome-specific risk of bias were assessed using the Quality in Prognosis Studies (QUIPS) tool. We rated the certainty of evidence using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE).
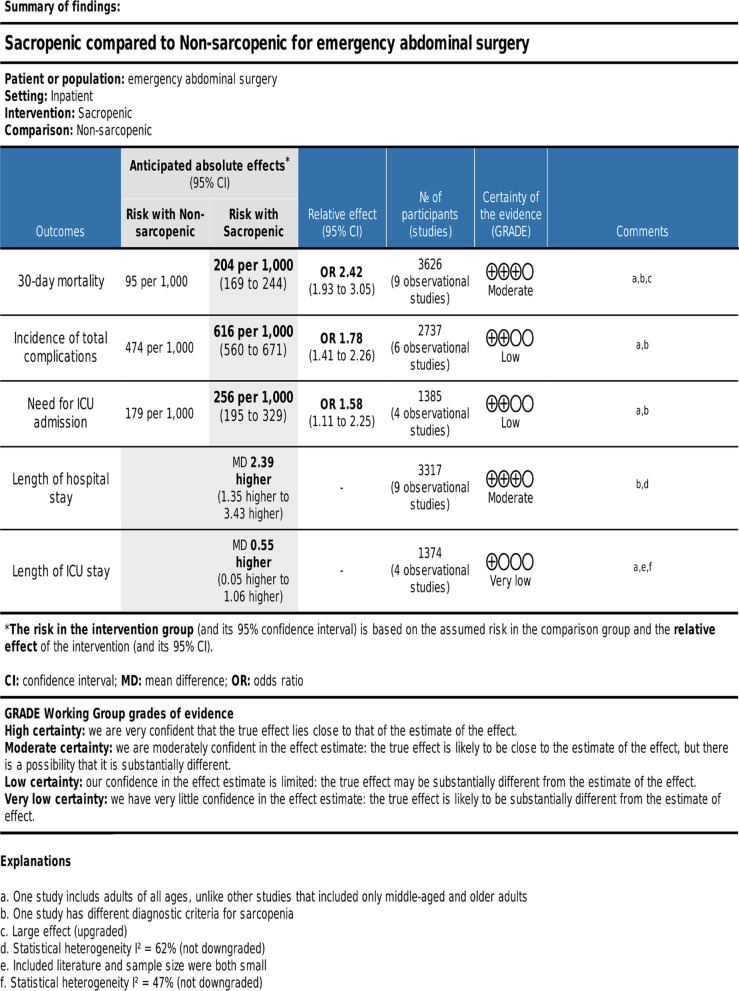
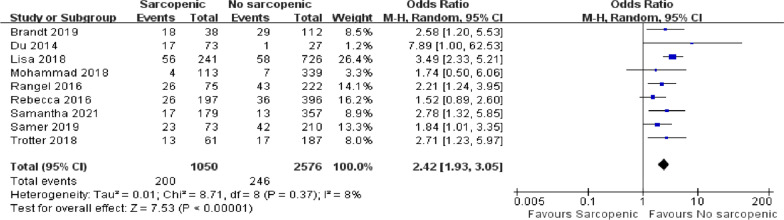
Result: A total of 11 eligible studies were included in this study. The results showed that patients with sarcopenia had a higher risk of death 30 days after surgery (OR = 2.42, 95% CI = 1.93-3.05, P < 0.00001). More patients were admitted to ICU after surgery (OR = 1.58, 95% CI = 1.11-2.25, P = 0.01). Both the ICU length of stay (MD = 0.55, 95% CI = 0.05-1.06, P = 0.03) and hospital length of stay (MD = 2.33, 95% CI = 1.33-3.32, P < 0.00001) were longer in the sarcopenia group. The incidence of postoperative complications was also significantly higher in patients with sarcopenia (OR = 1.78, 95% CI = 1.41-2.26, P < 0.00001).
Conclusion: In emergency laparotomy, sarcopenia was associated with increased 30-day postoperative mortality. Both the lengths of stay in the ICU and the total length of hospital stay were significantly higher than those in non-sarcopenic patients. Therefore, we concluded that sarcopenia can be used as a tool to identify preoperative high-risk patients, which can be considered to develop new postoperative risk prediction models. Registration number Registered on Prospero with the registration number of CRD42022300132.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


