Roberto De Icco, Gloria Vaghi, Marta Allena, Natascia Ghiotto, Elena Guaschino, Daniele Martinelli, Lara Ahmad, Michele Corrado, Federico Bighiani, Federica Tanganelli, Sara Bottiroli, Francescantonio Cammarota, Grazia Sances, Cristina Tassorelli
{"title":"3个月时MIDAS降低是否预示着伊瑞那单抗治疗的结果?一个真实的、开放标签的试验。","authors":"Roberto De Icco, Gloria Vaghi, Marta Allena, Natascia Ghiotto, Elena Guaschino, Daniele Martinelli, Lara Ahmad, Michele Corrado, Federico Bighiani, Federica Tanganelli, Sara Bottiroli, Francescantonio Cammarota, Grazia Sances, Cristina Tassorelli","doi":"10.1186/s10194-022-01480-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In Italy, monoclonal antibodies targeting the CGRP pathway are subsidized for the preventive treatment of high frequency and chronic migraine (CM) in patients with a MIgraine Disability ASsessment (MIDAS) score ≥ 11. Eligibility to treatment continuation requires a ≥ 50% MIDAS score reduction at three months (T3). In this study, we evaluate whether a ≥ 50% MIDAS score reduction at T3 is a reliable predictor of response to one-year erenumab treatment.</p><p><strong>Methods: </strong>In this prospective, open-label, real-world study, 77 CM patients were treated with erenumab 70-140 mg s.c. every 28 days for one year (T13). We collected the following variables: monthly migraine days (MMDs), monthly headache days (MHDs), days of acute medication intake, MIDAS, HIT-6, anxiety, depression, quality of life and allodynia. Response to erenumab was evaluated as: i) average reduction in MMDs during the 1-year treatment period; and ii) percentage of patients with ≥ 50% reduction in MMDs during the last 4 weeks after the 13<sup>th</sup> injection (Responders<sup>T13</sup>).</p><p><strong>Results: </strong>Erenumab induced a sustained reduction in MMDs, MHDs and intake of acute medications across the 12-month treatment period, with 64.9% of patients qualifying as Responders<sup>T13</sup>. At T3, 55.8% of patients reported a ≥ 50% reduction in MIDAS score (MIDAS<sup>Res</sup>) and 55.4% of patients reported a ≥ 50% reduction in MMDs (MMD<sup>Res</sup>). MIDAS<sup>Res</sup> and MMD<sup>Res</sup> patients showed a more pronounced reduction in MMDs during the 1-year treatment as compared to NON-MIDAS<sup>Res</sup> (MIDAS<sup>Res</sup>: T0: 23.5 ± 4.9 vs. T13: 7.7 ± 6.2; NON- MIDAS<sup>Res</sup>: T0: 21.6 ± 5.4 vs. T13: 11.3 ± 8.8, p = 0.045) and NON-MMD<sup>Res</sup> (MMD<sup>Res</sup>: T0: 23.0 ± 4.5 vs. T13: 6.6 ± 4.8; NON-MMD<sup>Res</sup>: T0: 22.3 ± 6.0 vs. T13: 12.7 ± 9.2, p < 0.001) groups. The percentage of Responders<sup>T13</sup> did not differ between MIDAS<sup>Res</sup> (74.4%) and NON-MIDAS<sup>Res</sup> (52.9%) patients (p = 0.058), while the percentage of Responders<sup>T13</sup> was higher in the MMD<sup>Res</sup> group (83.3%) when compared to NON-MMD<sup>Res</sup> (42.9%) (p = 0.001). MMD<sup>Res</sup> predicted the long-term outcome according to a multivariate analysis (Exp(B) = 7.128; p = 0.001), while MIDAS<sup>Res</sup> did not. Treatment discontinuation based on MIDAS<sup>Res</sup> would have early excluded 36.0% of Responders<sup>T13</sup>. Discontinuation based on \"either MIDAS<sup>Res</sup> or MMD<sup>Res</sup>\" would have excluded a lower percentage (16%) of Responders<sup>T13</sup>.</p><p><strong>Conclusion: </strong>MIDAS<sup>Res</sup> only partly reflects the 12-month outcome of erenumab treatment in CM, as it excludes more than one third of responders. A criterion based on the alternative consideration of ≥ 50% reduction in MIDAS score or MMDs in the first three months of treatment represents a more precise and inclusive option.</p><p><strong>Trial registration: </strong>The trial was retrospectively registered at www.</p><p><strong>Clinicaltrials: </strong>gov (NCT05442008). CGRP: Calcitonin Gene Related Peptide.</p><p><strong>Midas: </strong>MIgraine Disability Assessment. MMDs: monthly migraine days. MIDAS<sup>Res</sup>: Patients with a MIDAS score reduction of at least 50% at T3. MMD<sup>Res</sup>: Patients with a MMDs reduction of at least 50% at T3. Responder<sup>T13</sup>: Patients with a MMDs reduction from baseline of at least 50% in the last 4 weeks of observation period (after 13 erenumab administrations). T0: First erenumab administration. T3, T6, T9, T12: Follow-up visits at three, six, nine, and twelve months after first erenumab administration. T13: Last visit of the protocol.</p>","PeriodicalId":501630,"journal":{"name":"The Journal of Headache and Pain","volume":" ","pages":"123"},"PeriodicalIF":0.0000,"publicationDate":"2022-09-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9482180/pdf/","citationCount":"7","resultStr":"{\"title\":\"Does MIDAS reduction at 3 months predict the outcome of erenumab treatment? A real-world, open-label trial.\",\"authors\":\"Roberto De Icco, Gloria Vaghi, Marta Allena, Natascia Ghiotto, Elena Guaschino, Daniele Martinelli, Lara Ahmad, Michele Corrado, Federico Bighiani, Federica Tanganelli, Sara Bottiroli, Francescantonio Cammarota, Grazia Sances, Cristina Tassorelli\",\"doi\":\"10.1186/s10194-022-01480-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>In Italy, monoclonal antibodies targeting the CGRP pathway are subsidized for the preventive treatment of high frequency and chronic migraine (CM) in patients with a MIgraine Disability ASsessment (MIDAS) score ≥ 11. Eligibility to treatment continuation requires a ≥ 50% MIDAS score reduction at three months (T3). In this study, we evaluate whether a ≥ 50% MIDAS score reduction at T3 is a reliable predictor of response to one-year erenumab treatment.</p><p><strong>Methods: </strong>In this prospective, open-label, real-world study, 77 CM patients were treated with erenumab 70-140 mg s.c. every 28 days for one year (T13). We collected the following variables: monthly migraine days (MMDs), monthly headache days (MHDs), days of acute medication intake, MIDAS, HIT-6, anxiety, depression, quality of life and allodynia. Response to erenumab was evaluated as: i) average reduction in MMDs during the 1-year treatment period; and ii) percentage of patients with ≥ 50% reduction in MMDs during the last 4 weeks after the 13<sup>th</sup> injection (Responders<sup>T13</sup>).</p><p><strong>Results: </strong>Erenumab induced a sustained reduction in MMDs, MHDs and intake of acute medications across the 12-month treatment period, with 64.9% of patients qualifying as Responders<sup>T13</sup>. At T3, 55.8% of patients reported a ≥ 50% reduction in MIDAS score (MIDAS<sup>Res</sup>) and 55.4% of patients reported a ≥ 50% reduction in MMDs (MMD<sup>Res</sup>). MIDAS<sup>Res</sup> and MMD<sup>Res</sup> patients showed a more pronounced reduction in MMDs during the 1-year treatment as compared to NON-MIDAS<sup>Res</sup> (MIDAS<sup>Res</sup>: T0: 23.5 ± 4.9 vs. T13: 7.7 ± 6.2; NON- MIDAS<sup>Res</sup>: T0: 21.6 ± 5.4 vs. T13: 11.3 ± 8.8, p = 0.045) and NON-MMD<sup>Res</sup> (MMD<sup>Res</sup>: T0: 23.0 ± 4.5 vs. T13: 6.6 ± 4.8; NON-MMD<sup>Res</sup>: T0: 22.3 ± 6.0 vs. T13: 12.7 ± 9.2, p < 0.001) groups. The percentage of Responders<sup>T13</sup> did not differ between MIDAS<sup>Res</sup> (74.4%) and NON-MIDAS<sup>Res</sup> (52.9%) patients (p = 0.058), while the percentage of Responders<sup>T13</sup> was higher in the MMD<sup>Res</sup> group (83.3%) when compared to NON-MMD<sup>Res</sup> (42.9%) (p = 0.001). MMD<sup>Res</sup> predicted the long-term outcome according to a multivariate analysis (Exp(B) = 7.128; p = 0.001), while MIDAS<sup>Res</sup> did not. Treatment discontinuation based on MIDAS<sup>Res</sup> would have early excluded 36.0% of Responders<sup>T13</sup>. Discontinuation based on \\\"either MIDAS<sup>Res</sup> or MMD<sup>Res</sup>\\\" would have excluded a lower percentage (16%) of Responders<sup>T13</sup>.</p><p><strong>Conclusion: </strong>MIDAS<sup>Res</sup> only partly reflects the 12-month outcome of erenumab treatment in CM, as it excludes more than one third of responders. A criterion based on the alternative consideration of ≥ 50% reduction in MIDAS score or MMDs in the first three months of treatment represents a more precise and inclusive option.</p><p><strong>Trial registration: </strong>The trial was retrospectively registered at www.</p><p><strong>Clinicaltrials: </strong>gov (NCT05442008). CGRP: Calcitonin Gene Related Peptide.</p><p><strong>Midas: </strong>MIgraine Disability Assessment. MMDs: monthly migraine days. MIDAS<sup>Res</sup>: Patients with a MIDAS score reduction of at least 50% at T3. MMD<sup>Res</sup>: Patients with a MMDs reduction of at least 50% at T3. Responder<sup>T13</sup>: Patients with a MMDs reduction from baseline of at least 50% in the last 4 weeks of observation period (after 13 erenumab administrations). T0: First erenumab administration. T3, T6, T9, T12: Follow-up visits at three, six, nine, and twelve months after first erenumab administration. T13: Last visit of the protocol.</p>\",\"PeriodicalId\":501630,\"journal\":{\"name\":\"The Journal of Headache and Pain\",\"volume\":\" \",\"pages\":\"123\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-09-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9482180/pdf/\",\"citationCount\":\"7\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Journal of Headache and Pain\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s10194-022-01480-2\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Journal of Headache and Pain","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s10194-022-01480-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Does MIDAS reduction at 3 months predict the outcome of erenumab treatment? A real-world, open-label trial.
Background: In Italy, monoclonal antibodies targeting the CGRP pathway are subsidized for the preventive treatment of high frequency and chronic migraine (CM) in patients with a MIgraine Disability ASsessment (MIDAS) score ≥ 11. Eligibility to treatment continuation requires a ≥ 50% MIDAS score reduction at three months (T3). In this study, we evaluate whether a ≥ 50% MIDAS score reduction at T3 is a reliable predictor of response to one-year erenumab treatment.
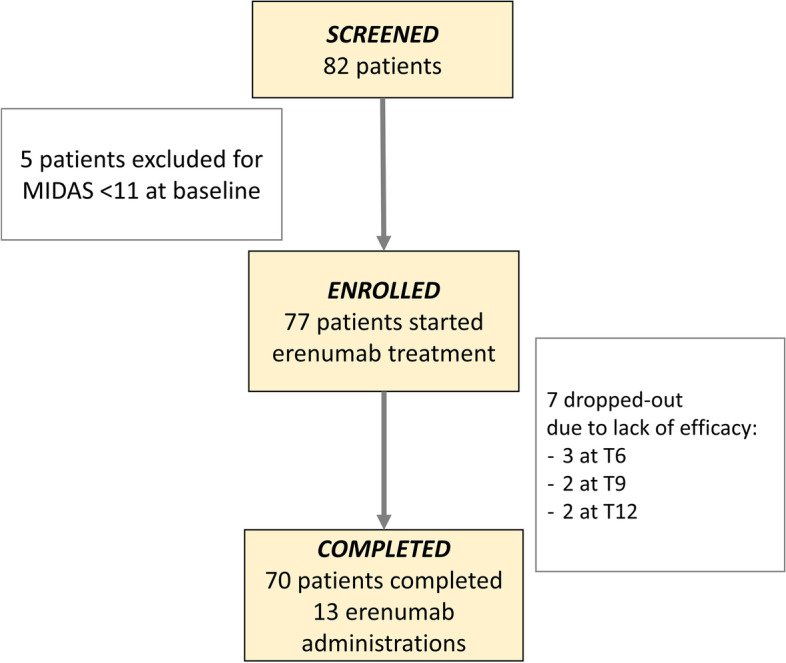
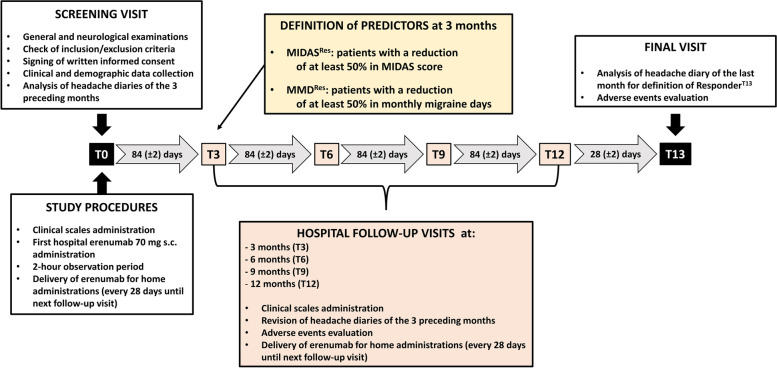
Methods: In this prospective, open-label, real-world study, 77 CM patients were treated with erenumab 70-140 mg s.c. every 28 days for one year (T13). We collected the following variables: monthly migraine days (MMDs), monthly headache days (MHDs), days of acute medication intake, MIDAS, HIT-6, anxiety, depression, quality of life and allodynia. Response to erenumab was evaluated as: i) average reduction in MMDs during the 1-year treatment period; and ii) percentage of patients with ≥ 50% reduction in MMDs during the last 4 weeks after the 13th injection (RespondersT13).
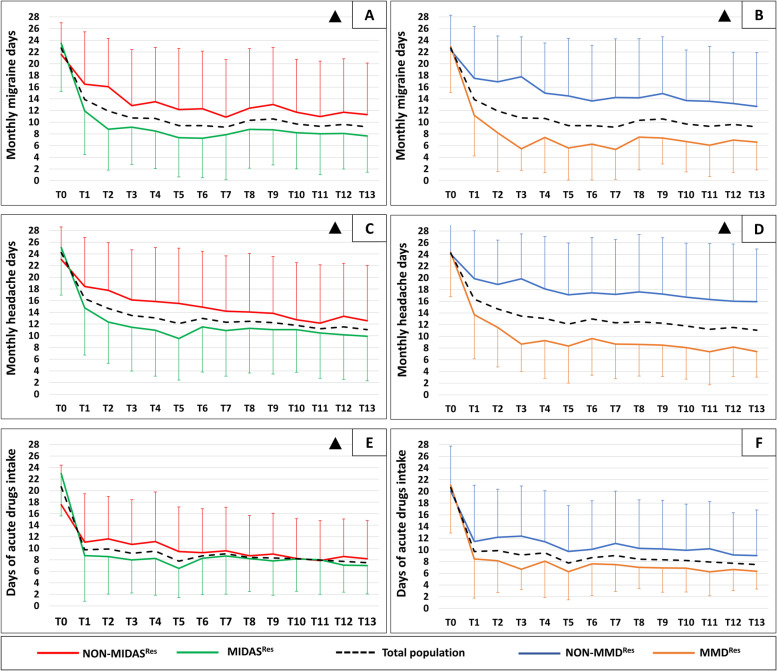
Results: Erenumab induced a sustained reduction in MMDs, MHDs and intake of acute medications across the 12-month treatment period, with 64.9% of patients qualifying as RespondersT13. At T3, 55.8% of patients reported a ≥ 50% reduction in MIDAS score (MIDASRes) and 55.4% of patients reported a ≥ 50% reduction in MMDs (MMDRes). MIDASRes and MMDRes patients showed a more pronounced reduction in MMDs during the 1-year treatment as compared to NON-MIDASRes (MIDASRes: T0: 23.5 ± 4.9 vs. T13: 7.7 ± 6.2; NON- MIDASRes: T0: 21.6 ± 5.4 vs. T13: 11.3 ± 8.8, p = 0.045) and NON-MMDRes (MMDRes: T0: 23.0 ± 4.5 vs. T13: 6.6 ± 4.8; NON-MMDRes: T0: 22.3 ± 6.0 vs. T13: 12.7 ± 9.2, p < 0.001) groups. The percentage of RespondersT13 did not differ between MIDASRes (74.4%) and NON-MIDASRes (52.9%) patients (p = 0.058), while the percentage of RespondersT13 was higher in the MMDRes group (83.3%) when compared to NON-MMDRes (42.9%) (p = 0.001). MMDRes predicted the long-term outcome according to a multivariate analysis (Exp(B) = 7.128; p = 0.001), while MIDASRes did not. Treatment discontinuation based on MIDASRes would have early excluded 36.0% of RespondersT13. Discontinuation based on "either MIDASRes or MMDRes" would have excluded a lower percentage (16%) of RespondersT13.
Conclusion: MIDASRes only partly reflects the 12-month outcome of erenumab treatment in CM, as it excludes more than one third of responders. A criterion based on the alternative consideration of ≥ 50% reduction in MIDAS score or MMDs in the first three months of treatment represents a more precise and inclusive option.
Trial registration: The trial was retrospectively registered at www.
Clinicaltrials: gov (NCT05442008). CGRP: Calcitonin Gene Related Peptide.
Midas: MIgraine Disability Assessment. MMDs: monthly migraine days. MIDASRes: Patients with a MIDAS score reduction of at least 50% at T3. MMDRes: Patients with a MMDs reduction of at least 50% at T3. ResponderT13: Patients with a MMDs reduction from baseline of at least 50% in the last 4 weeks of observation period (after 13 erenumab administrations). T0: First erenumab administration. T3, T6, T9, T12: Follow-up visits at three, six, nine, and twelve months after first erenumab administration. T13: Last visit of the protocol.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


