Isabel Mosquera, Andre Ilbawi, Richard Muwonge, Partha Basu, Andre L Carvalho
{"title":"脆弱国家的癌症负担和癌症控制措施现状:31个国家的比较分析。","authors":"Isabel Mosquera, Andre Ilbawi, Richard Muwonge, Partha Basu, Andre L Carvalho","doi":"10.1016/S2214-109X(22)00331-X","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Information on cancer statistics and cancer control policies is limited in fragile states. This paper describes the cancer burden and status of cancer control measures in these countries.</p><p><strong>Methods: </strong>In this comparative analysis, fragile states presenting with a Fragile States Index (FSI) score of 90·0 or more (alert for fragility) for at least 10 years during the 2006-20 period were selected. States with fewer than 10 years of data were selected if they were in alert for fragility during all years. Information on cancer burden, prevalence of cancer risk factors, population-attributable fraction, and on political commitment, health financing, and health system capacity was collected. Cancer incidence and mortality was calculated on the basis of data from population-based cancer registries, estimated with modelling that used mortality-to-incidence ratios and incidence-to-mortality ratios derived from cancer registries in neighbouring countries, or average of rates in selected neighbouring countries. For statistical comparison, fragile states were grouped according to the annual percent change (APC) of the FSI, with group 1 showing an increasing fragility trend (APC 0·2% or higher), group 2 a relatively stable fragility trend (APC between 0·2% and -0·2%), and group 3 a decreasing fragility trend (APC of -0·2% or lower).</p><p><strong>Findings: </strong>Overall, the estimated cancer burden in the 31 selected fragile states was lower than worldwide rates, except for cervical and prostate cancer. Cancer cases were attributed to infections (22·40% in group 1, 21·20% in group 2, and 18·80% in group 3) at a higher proportion in fragile states than globally (13·0%). Group 1 and 2 showed a significantly higher exposure to household air pollution (97·70% in group 1 and 94·90% in group 2), whereas current tobacco use in men increased from group 1 to group 3, with lung cancer incidence and mortality being higher in group 3. However, 25 countries had implemented only one or no MPOWER measures for tobacco control. Countries showed an out-of-pocket expenditure of 48·72% in group 1, 42·68% in group 2, and 51·07% in group 3, and only half of the countries had an updated cancer control plan or cancer management guidelines.</p><p><strong>Interpretation: </strong>Fragile states have started the epidemiological transition but are still not implementing enough cancer control measures. There is a need to develop reliable cancer control plans and guidelines, and to create financial mechanisms for implementation.</p><p><strong>Funding: </strong>None.</p><p><strong>Translations: </strong>For the Arabic and French translations of the abstract see Supplementary Materials section.</p>","PeriodicalId":153380,"journal":{"name":"The Lancet. Global health","volume":" ","pages":"e1443-e1452"},"PeriodicalIF":0.0000,"publicationDate":"2022-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9638035/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cancer burden and status of cancer control measures in fragile states: a comparative analysis of 31 countries.\",\"authors\":\"Isabel Mosquera, Andre Ilbawi, Richard Muwonge, Partha Basu, Andre L Carvalho\",\"doi\":\"10.1016/S2214-109X(22)00331-X\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Information on cancer statistics and cancer control policies is limited in fragile states. This paper describes the cancer burden and status of cancer control measures in these countries.</p><p><strong>Methods: </strong>In this comparative analysis, fragile states presenting with a Fragile States Index (FSI) score of 90·0 or more (alert for fragility) for at least 10 years during the 2006-20 period were selected. States with fewer than 10 years of data were selected if they were in alert for fragility during all years. Information on cancer burden, prevalence of cancer risk factors, population-attributable fraction, and on political commitment, health financing, and health system capacity was collected. Cancer incidence and mortality was calculated on the basis of data from population-based cancer registries, estimated with modelling that used mortality-to-incidence ratios and incidence-to-mortality ratios derived from cancer registries in neighbouring countries, or average of rates in selected neighbouring countries. For statistical comparison, fragile states were grouped according to the annual percent change (APC) of the FSI, with group 1 showing an increasing fragility trend (APC 0·2% or higher), group 2 a relatively stable fragility trend (APC between 0·2% and -0·2%), and group 3 a decreasing fragility trend (APC of -0·2% or lower).</p><p><strong>Findings: </strong>Overall, the estimated cancer burden in the 31 selected fragile states was lower than worldwide rates, except for cervical and prostate cancer. Cancer cases were attributed to infections (22·40% in group 1, 21·20% in group 2, and 18·80% in group 3) at a higher proportion in fragile states than globally (13·0%). Group 1 and 2 showed a significantly higher exposure to household air pollution (97·70% in group 1 and 94·90% in group 2), whereas current tobacco use in men increased from group 1 to group 3, with lung cancer incidence and mortality being higher in group 3. However, 25 countries had implemented only one or no MPOWER measures for tobacco control. Countries showed an out-of-pocket expenditure of 48·72% in group 1, 42·68% in group 2, and 51·07% in group 3, and only half of the countries had an updated cancer control plan or cancer management guidelines.</p><p><strong>Interpretation: </strong>Fragile states have started the epidemiological transition but are still not implementing enough cancer control measures. There is a need to develop reliable cancer control plans and guidelines, and to create financial mechanisms for implementation.</p><p><strong>Funding: </strong>None.</p><p><strong>Translations: </strong>For the Arabic and French translations of the abstract see Supplementary Materials section.</p>\",\"PeriodicalId\":153380,\"journal\":{\"name\":\"The Lancet. Global health\",\"volume\":\" \",\"pages\":\"e1443-e1452\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9638035/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Lancet. Global health\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1016/S2214-109X(22)00331-X\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Lancet. Global health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1016/S2214-109X(22)00331-X","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Cancer burden and status of cancer control measures in fragile states: a comparative analysis of 31 countries.
Background: Information on cancer statistics and cancer control policies is limited in fragile states. This paper describes the cancer burden and status of cancer control measures in these countries.
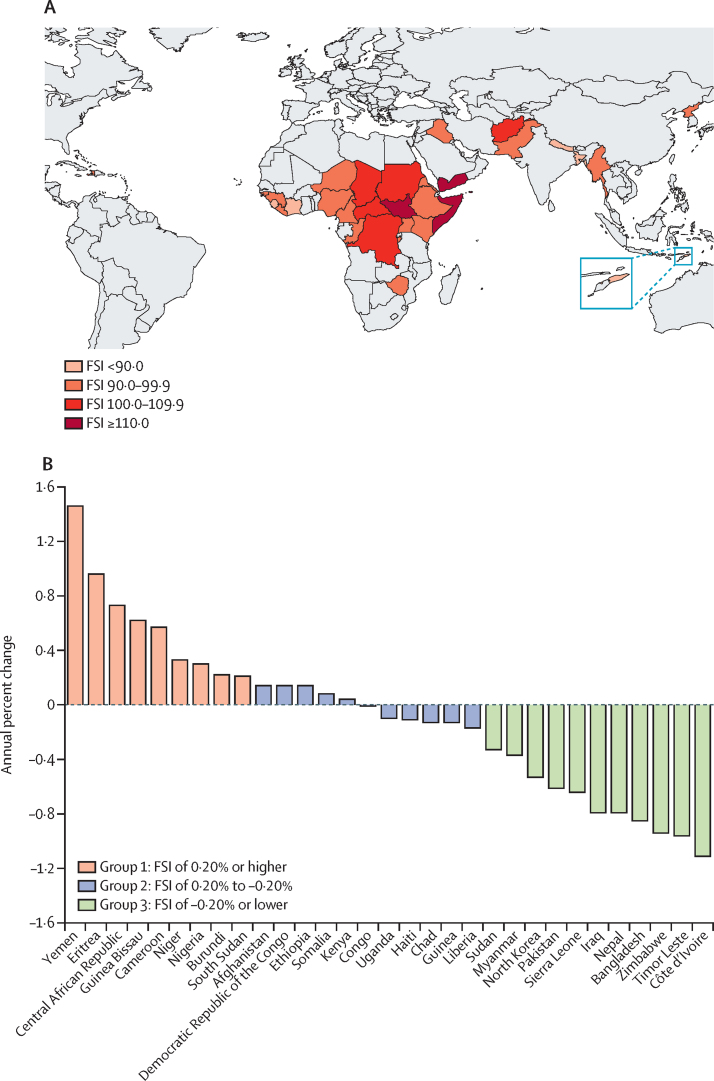
Methods: In this comparative analysis, fragile states presenting with a Fragile States Index (FSI) score of 90·0 or more (alert for fragility) for at least 10 years during the 2006-20 period were selected. States with fewer than 10 years of data were selected if they were in alert for fragility during all years. Information on cancer burden, prevalence of cancer risk factors, population-attributable fraction, and on political commitment, health financing, and health system capacity was collected. Cancer incidence and mortality was calculated on the basis of data from population-based cancer registries, estimated with modelling that used mortality-to-incidence ratios and incidence-to-mortality ratios derived from cancer registries in neighbouring countries, or average of rates in selected neighbouring countries. For statistical comparison, fragile states were grouped according to the annual percent change (APC) of the FSI, with group 1 showing an increasing fragility trend (APC 0·2% or higher), group 2 a relatively stable fragility trend (APC between 0·2% and -0·2%), and group 3 a decreasing fragility trend (APC of -0·2% or lower).
Findings: Overall, the estimated cancer burden in the 31 selected fragile states was lower than worldwide rates, except for cervical and prostate cancer. Cancer cases were attributed to infections (22·40% in group 1, 21·20% in group 2, and 18·80% in group 3) at a higher proportion in fragile states than globally (13·0%). Group 1 and 2 showed a significantly higher exposure to household air pollution (97·70% in group 1 and 94·90% in group 2), whereas current tobacco use in men increased from group 1 to group 3, with lung cancer incidence and mortality being higher in group 3. However, 25 countries had implemented only one or no MPOWER measures for tobacco control. Countries showed an out-of-pocket expenditure of 48·72% in group 1, 42·68% in group 2, and 51·07% in group 3, and only half of the countries had an updated cancer control plan or cancer management guidelines.
Interpretation: Fragile states have started the epidemiological transition but are still not implementing enough cancer control measures. There is a need to develop reliable cancer control plans and guidelines, and to create financial mechanisms for implementation.
Funding: None.
Translations: For the Arabic and French translations of the abstract see Supplementary Materials section.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


