Mehmet Celal Öztürk, Murat Küçük, Yasin Levent Uğur, Bilgin Cömert, Ali Necati Gökmen, Begüm Ergan
{"title":"纤维支气管镜对危重重症急性呼吸窘迫综合征患者气道压力释放通气模式安全性的初步研究。","authors":"Mehmet Celal Öztürk, Murat Küçük, Yasin Levent Uğur, Bilgin Cömert, Ali Necati Gökmen, Begüm Ergan","doi":"10.5152/TurkThoracJ.2022.21241","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The most appropriate ventilatory mode during fiberoptic bronchoscopy is still not yet known clearly for patients with acute respiratory distress syndrome. Airway pressure release ventilation is used as a recovery treatment for patients with severe acute respiratory distress syndrome. In this study, the aim was to evaluate the safety of the fiberoptic bronchoscopy process in patients with severe acute respiratory distress syndrome ventilated with airway pressure release ventilation mode and its effect on gas exchange and respiratory mechanics.</p><p><strong>Material and methods: </strong>Single-center retrospective observational study was performed in the intensive care unit of a tertiary referral center from September 2018 to November 2019. Patients with severe ARDS ventilated with APRV mode and undergoing FB were included. Fiberoptic bronchoscopy was performed by an expert intensivist-pulmonologist. All ventilator parameters set by the clinician were kept stable, and no change was made other than O2 concentration. The mechanical ventilation parameters and arterial blood gas values before and after the procedure and fiberoptic bronchoscopy-related complications were recorded for the first 24 hours.</p><p><strong>Results: </strong>A total of 14 acute respiratory distress syndrome patients who were ventilated with airway pressure release ventilation were enrolled. No significant deteriorations were detected in gas exchange, pulmonary compliance, and airway resistance values in our case series. It was observed that a small reduction in PaO2 and an increase in PaCO2 were present after the 1st hour; however, both were returned to baseline values in the 24th hour. Only 1 patient developed fiberoptic bronchoscopy-induced hypoxemia (7.1%). Complications, such as fiberoptic bronchoscopy-induced barotrauma, pneumothorax, hemodynamic deterioration, and bleeding, were not detected.</p><p><strong>Conclusion: </strong>According to our preliminary findings, performing fiberoptic bronchoscopy under airway pressure release ventilation mode by an experienced bronchoscopist does not bring additional complication risks in patients with severe acute respiratory distress syndrome.</p>","PeriodicalId":37452,"journal":{"name":"Turkish Thoracic Journal","volume":" ","pages":"403-408"},"PeriodicalIF":0.8000,"publicationDate":"2022-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b2/8b/ttj-23-6-403.PMC9682956.pdf","citationCount":"1","resultStr":"{\"title\":\"The Safety of Fiberoptic Bronchoscopy in Airway Pressure Release Ventilation Mode in Critically Ill Patients with Severe Acute Respiratory Distress Syndrome: A Preliminary Study.\",\"authors\":\"Mehmet Celal Öztürk, Murat Küçük, Yasin Levent Uğur, Bilgin Cömert, Ali Necati Gökmen, Begüm Ergan\",\"doi\":\"10.5152/TurkThoracJ.2022.21241\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>The most appropriate ventilatory mode during fiberoptic bronchoscopy is still not yet known clearly for patients with acute respiratory distress syndrome. Airway pressure release ventilation is used as a recovery treatment for patients with severe acute respiratory distress syndrome. In this study, the aim was to evaluate the safety of the fiberoptic bronchoscopy process in patients with severe acute respiratory distress syndrome ventilated with airway pressure release ventilation mode and its effect on gas exchange and respiratory mechanics.</p><p><strong>Material and methods: </strong>Single-center retrospective observational study was performed in the intensive care unit of a tertiary referral center from September 2018 to November 2019. Patients with severe ARDS ventilated with APRV mode and undergoing FB were included. Fiberoptic bronchoscopy was performed by an expert intensivist-pulmonologist. All ventilator parameters set by the clinician were kept stable, and no change was made other than O2 concentration. The mechanical ventilation parameters and arterial blood gas values before and after the procedure and fiberoptic bronchoscopy-related complications were recorded for the first 24 hours.</p><p><strong>Results: </strong>A total of 14 acute respiratory distress syndrome patients who were ventilated with airway pressure release ventilation were enrolled. No significant deteriorations were detected in gas exchange, pulmonary compliance, and airway resistance values in our case series. It was observed that a small reduction in PaO2 and an increase in PaCO2 were present after the 1st hour; however, both were returned to baseline values in the 24th hour. Only 1 patient developed fiberoptic bronchoscopy-induced hypoxemia (7.1%). Complications, such as fiberoptic bronchoscopy-induced barotrauma, pneumothorax, hemodynamic deterioration, and bleeding, were not detected.</p><p><strong>Conclusion: </strong>According to our preliminary findings, performing fiberoptic bronchoscopy under airway pressure release ventilation mode by an experienced bronchoscopist does not bring additional complication risks in patients with severe acute respiratory distress syndrome.</p>\",\"PeriodicalId\":37452,\"journal\":{\"name\":\"Turkish Thoracic Journal\",\"volume\":\" \",\"pages\":\"403-408\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2022-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b2/8b/ttj-23-6-403.PMC9682956.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Turkish Thoracic Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5152/TurkThoracJ.2022.21241\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Turkish Thoracic Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5152/TurkThoracJ.2022.21241","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
The Safety of Fiberoptic Bronchoscopy in Airway Pressure Release Ventilation Mode in Critically Ill Patients with Severe Acute Respiratory Distress Syndrome: A Preliminary Study.
Objective: The most appropriate ventilatory mode during fiberoptic bronchoscopy is still not yet known clearly for patients with acute respiratory distress syndrome. Airway pressure release ventilation is used as a recovery treatment for patients with severe acute respiratory distress syndrome. In this study, the aim was to evaluate the safety of the fiberoptic bronchoscopy process in patients with severe acute respiratory distress syndrome ventilated with airway pressure release ventilation mode and its effect on gas exchange and respiratory mechanics.
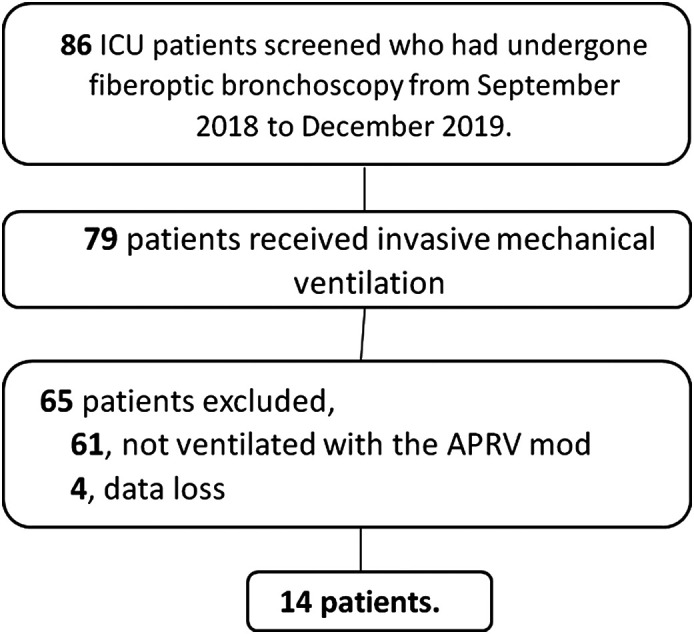
Material and methods: Single-center retrospective observational study was performed in the intensive care unit of a tertiary referral center from September 2018 to November 2019. Patients with severe ARDS ventilated with APRV mode and undergoing FB were included. Fiberoptic bronchoscopy was performed by an expert intensivist-pulmonologist. All ventilator parameters set by the clinician were kept stable, and no change was made other than O2 concentration. The mechanical ventilation parameters and arterial blood gas values before and after the procedure and fiberoptic bronchoscopy-related complications were recorded for the first 24 hours.
Results: A total of 14 acute respiratory distress syndrome patients who were ventilated with airway pressure release ventilation were enrolled. No significant deteriorations were detected in gas exchange, pulmonary compliance, and airway resistance values in our case series. It was observed that a small reduction in PaO2 and an increase in PaCO2 were present after the 1st hour; however, both were returned to baseline values in the 24th hour. Only 1 patient developed fiberoptic bronchoscopy-induced hypoxemia (7.1%). Complications, such as fiberoptic bronchoscopy-induced barotrauma, pneumothorax, hemodynamic deterioration, and bleeding, were not detected.
Conclusion: According to our preliminary findings, performing fiberoptic bronchoscopy under airway pressure release ventilation mode by an experienced bronchoscopist does not bring additional complication risks in patients with severe acute respiratory distress syndrome.
期刊介绍:
Turkish Thoracic Journal (Turk Thorac J) is the double-blind, peer-reviewed, open access, international publication organ of Turkish Thoracic Society. The journal is a quarterly publication, published on January, April, July, and October and its publication language is English. Turkish Thoracic Journal started its publication life following the merger of two journals which were published under the titles “Turkish Respiratory Journal” and “Toraks Journal” until 2007. Archives of both journals were passed on to the Turkish Thoracic Journal. The aim of the journal is to convey scientific developments and to create a dynamic discussion platform about pulmonary diseases. With this intent, the journal accepts articles from all related scientific areas that address adult and pediatric pulmonary diseases, as well as thoracic imaging, environmental and occupational disorders, intensive care, sleep disorders and thoracic surgery. Clinical and research articles, reviews, statements of agreement or disagreement on controversial issues, national and international consensus reports, abstracts and comments of important international articles, interesting case reports, writings related to clinical and practical applications, letters to the editor, and editorials are accepted.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


