Sebastien Kenmoe, Etienne Atenguena Okobalemba, Guy Roussel Takuissu, Jean Thierry Ebogo-Belobo, Martin Gael Oyono, Jeannette Nina Magoudjou-Pekam, Ginette Irma Kame-Ngasse, Jean Bosco Taya-Fokou, Chris Andre Mbongue Mikangue, Raoul Kenfack-Momo, Donatien Serge Mbaga, Arnol Bowo-Ngandji, Cyprien Kengne-Ndé, Seraphine Nkie Esemu, Richard Njouom, Lucy Ndip
{"title":"早期病毒性下呼吸道感染与随后哮喘发展之间的关系。","authors":"Sebastien Kenmoe, Etienne Atenguena Okobalemba, Guy Roussel Takuissu, Jean Thierry Ebogo-Belobo, Martin Gael Oyono, Jeannette Nina Magoudjou-Pekam, Ginette Irma Kame-Ngasse, Jean Bosco Taya-Fokou, Chris Andre Mbongue Mikangue, Raoul Kenfack-Momo, Donatien Serge Mbaga, Arnol Bowo-Ngandji, Cyprien Kengne-Ndé, Seraphine Nkie Esemu, Richard Njouom, Lucy Ndip","doi":"10.5492/wjccm.v11.i4.298","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The association between hospitalization for human respiratory syncytial virus (HRSV) bronchiolitis in early childhood and subsequent asthma is well established. The long-term prognosis for non-bronchiolitis lower respiratory tract infections (LRTI) caused by viruses different from HRSV and rhinovirus, on the other hand, has received less interest.</p><p><strong>Aim: </strong>To investigate the relationship between infant LRTI and later asthma and examine the influence of confounding factors.</p><p><strong>Methods: </strong>The PubMed and Global Index Medicus bibliographic databases were used to search for articles published up to October 2021 for this systematic review. We included cohort studies comparing the incidence of asthma between patients with and without LRTI at ≤ 2 years regardless of the virus responsible. The meta-analysis was performed using the random effects model. Sources of heterogeneity were assessed by stratified analyses.</p><p><strong>Results: </strong>This review included 15 articles (18 unique studies) that met the inclusion criteria. LRTIs at ≤ 2 years were associated with an increased risk of subsequent asthma up to 20 years [odds ratio (OR) = 5.0, 95%CI: 3.3-7.5], with doctor-diagnosed asthma (OR = 5.3, 95%CI: 3.3-8.6), current asthma (OR = 5.4, 95%CI: 2.7-10.6), and current medication for asthma (OR = 1.2, 95%CI: 0.7-3.9). Our overall estimates were not affected by publication bias (<i>P</i> = 0.671), but there was significant heterogeneity [<i>I</i> <sup>2</sup> = 58.8% (30.6-75.5)]. Compared to studies with hospitalized controls without LRTI, those with ambulatory controls had a significantly higher strength of association between LRTIs and subsequent asthma. The strength of the association between LRTIs and later asthma varied significantly by country and age at the time of the interview. The sensitivity analyses including only studies with similar proportions of confounding factors (gender, age at LRTI development, age at interview, gestational age, birth weight, weight, height, smoking exposure, crowding, family history of atopy, and family history of asthma) between cases and controls did not alter the overall estimates.</p><p><strong>Conclusion: </strong>Regardless of the causative virus and confounding factors, viral LRTIs in children < 2 years are associated with an increased risk of developing a subsequent asthma. Parents and pediatricians should be informed of this risk.</p>","PeriodicalId":66959,"journal":{"name":"世界危重病急救学杂志(英文版)","volume":"11 4","pages":"298-310"},"PeriodicalIF":0.0000,"publicationDate":"2022-07-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/81/78/WJCCM-11-298.PMC9305678.pdf","citationCount":"0","resultStr":"{\"title\":\"Association between early viral lower respiratory tract infections and subsequent asthma development.\",\"authors\":\"Sebastien Kenmoe, Etienne Atenguena Okobalemba, Guy Roussel Takuissu, Jean Thierry Ebogo-Belobo, Martin Gael Oyono, Jeannette Nina Magoudjou-Pekam, Ginette Irma Kame-Ngasse, Jean Bosco Taya-Fokou, Chris Andre Mbongue Mikangue, Raoul Kenfack-Momo, Donatien Serge Mbaga, Arnol Bowo-Ngandji, Cyprien Kengne-Ndé, Seraphine Nkie Esemu, Richard Njouom, Lucy Ndip\",\"doi\":\"10.5492/wjccm.v11.i4.298\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The association between hospitalization for human respiratory syncytial virus (HRSV) bronchiolitis in early childhood and subsequent asthma is well established. The long-term prognosis for non-bronchiolitis lower respiratory tract infections (LRTI) caused by viruses different from HRSV and rhinovirus, on the other hand, has received less interest.</p><p><strong>Aim: </strong>To investigate the relationship between infant LRTI and later asthma and examine the influence of confounding factors.</p><p><strong>Methods: </strong>The PubMed and Global Index Medicus bibliographic databases were used to search for articles published up to October 2021 for this systematic review. We included cohort studies comparing the incidence of asthma between patients with and without LRTI at ≤ 2 years regardless of the virus responsible. The meta-analysis was performed using the random effects model. Sources of heterogeneity were assessed by stratified analyses.</p><p><strong>Results: </strong>This review included 15 articles (18 unique studies) that met the inclusion criteria. LRTIs at ≤ 2 years were associated with an increased risk of subsequent asthma up to 20 years [odds ratio (OR) = 5.0, 95%CI: 3.3-7.5], with doctor-diagnosed asthma (OR = 5.3, 95%CI: 3.3-8.6), current asthma (OR = 5.4, 95%CI: 2.7-10.6), and current medication for asthma (OR = 1.2, 95%CI: 0.7-3.9). Our overall estimates were not affected by publication bias (<i>P</i> = 0.671), but there was significant heterogeneity [<i>I</i> <sup>2</sup> = 58.8% (30.6-75.5)]. Compared to studies with hospitalized controls without LRTI, those with ambulatory controls had a significantly higher strength of association between LRTIs and subsequent asthma. The strength of the association between LRTIs and later asthma varied significantly by country and age at the time of the interview. The sensitivity analyses including only studies with similar proportions of confounding factors (gender, age at LRTI development, age at interview, gestational age, birth weight, weight, height, smoking exposure, crowding, family history of atopy, and family history of asthma) between cases and controls did not alter the overall estimates.</p><p><strong>Conclusion: </strong>Regardless of the causative virus and confounding factors, viral LRTIs in children < 2 years are associated with an increased risk of developing a subsequent asthma. Parents and pediatricians should be informed of this risk.</p>\",\"PeriodicalId\":66959,\"journal\":{\"name\":\"世界危重病急救学杂志(英文版)\",\"volume\":\"11 4\",\"pages\":\"298-310\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-07-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/81/78/WJCCM-11-298.PMC9305678.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"世界危重病急救学杂志(英文版)\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5492/wjccm.v11.i4.298\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界危重病急救学杂志(英文版)","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5492/wjccm.v11.i4.298","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Association between early viral lower respiratory tract infections and subsequent asthma development.
Background: The association between hospitalization for human respiratory syncytial virus (HRSV) bronchiolitis in early childhood and subsequent asthma is well established. The long-term prognosis for non-bronchiolitis lower respiratory tract infections (LRTI) caused by viruses different from HRSV and rhinovirus, on the other hand, has received less interest.
Aim: To investigate the relationship between infant LRTI and later asthma and examine the influence of confounding factors.
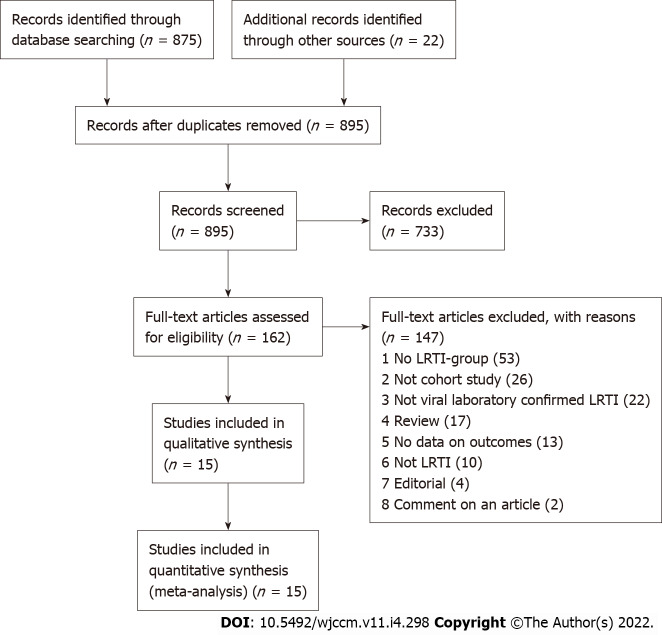
Methods: The PubMed and Global Index Medicus bibliographic databases were used to search for articles published up to October 2021 for this systematic review. We included cohort studies comparing the incidence of asthma between patients with and without LRTI at ≤ 2 years regardless of the virus responsible. The meta-analysis was performed using the random effects model. Sources of heterogeneity were assessed by stratified analyses.
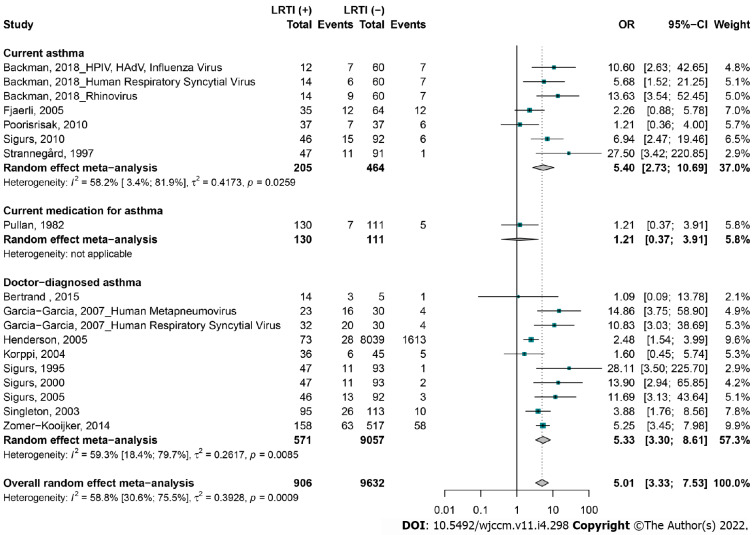
Results: This review included 15 articles (18 unique studies) that met the inclusion criteria. LRTIs at ≤ 2 years were associated with an increased risk of subsequent asthma up to 20 years [odds ratio (OR) = 5.0, 95%CI: 3.3-7.5], with doctor-diagnosed asthma (OR = 5.3, 95%CI: 3.3-8.6), current asthma (OR = 5.4, 95%CI: 2.7-10.6), and current medication for asthma (OR = 1.2, 95%CI: 0.7-3.9). Our overall estimates were not affected by publication bias (P = 0.671), but there was significant heterogeneity [I2 = 58.8% (30.6-75.5)]. Compared to studies with hospitalized controls without LRTI, those with ambulatory controls had a significantly higher strength of association between LRTIs and subsequent asthma. The strength of the association between LRTIs and later asthma varied significantly by country and age at the time of the interview. The sensitivity analyses including only studies with similar proportions of confounding factors (gender, age at LRTI development, age at interview, gestational age, birth weight, weight, height, smoking exposure, crowding, family history of atopy, and family history of asthma) between cases and controls did not alter the overall estimates.
Conclusion: Regardless of the causative virus and confounding factors, viral LRTIs in children < 2 years are associated with an increased risk of developing a subsequent asthma. Parents and pediatricians should be informed of this risk.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


