Jaydip Ray Chaudhuri, Jui Jade Bagul, Alluri Swathi, Bhim Sen Singhal, N Chakradhar Reddy, Kiran Kumar Vallam
{"title":"髓鞘少突胶质细胞糖蛋白抗体相关疾病表现为颅内高血压1例","authors":"Jaydip Ray Chaudhuri, Jui Jade Bagul, Alluri Swathi, Bhim Sen Singhal, N Chakradhar Reddy, Kiran Kumar Vallam","doi":"10.1212/NXI.0000000000200020","DOIUrl":null,"url":null,"abstract":"<p><p>The production of autoantibodies against myelin oligodendrocyte glycoprotein (MOG) can cause a spectrum of autoimmune disorders, including optic neuritis, transverse myelitis, brainstem encephalitis, and acute disseminated encephalomyelitis. In this study, we present the case of a 19-year-old woman with an unusual clinical presentation of intracranial hypertension (IH) and bilateral papilledema. The patient presented with symptoms of increased intracranial pressure, which followed a relapsing, remitting course over several months. Serial CSF studies showed an increased opening pressure during clinical relapses. The CSF and serum tested positive for MOG immunoglobulin G antibodies. Contrast-enhanced MRI of the brain showed mild meningeal enhancement in the left parietal region with subtle underlying cortical hyperintensities, indicating possible fluid-attenuated inversion recovery variable unilateral enhancement of the leptomeninges. The patient responded well to immunosuppressive therapy using rituximab. The presentation of MOG antibody-associated disease (MOGAD) as IH without optic neuritis is rare. This report presents the first description of a relapsing remitting course presenting each time with only symptoms of raised intracranial pressure, without developing any typical clinical manifestations of MOGAD.</p>","PeriodicalId":520720,"journal":{"name":"Neurology(R) neuroimmunology & neuroinflammation","volume":" ","pages":""},"PeriodicalIF":7.5000,"publicationDate":"2022-10-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/7f/3f/NXI-2022-200026.PMC9581460.pdf","citationCount":"2","resultStr":"{\"title\":\"Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease Presenting as Intracranial Hypertension: A Case Report.\",\"authors\":\"Jaydip Ray Chaudhuri, Jui Jade Bagul, Alluri Swathi, Bhim Sen Singhal, N Chakradhar Reddy, Kiran Kumar Vallam\",\"doi\":\"10.1212/NXI.0000000000200020\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The production of autoantibodies against myelin oligodendrocyte glycoprotein (MOG) can cause a spectrum of autoimmune disorders, including optic neuritis, transverse myelitis, brainstem encephalitis, and acute disseminated encephalomyelitis. In this study, we present the case of a 19-year-old woman with an unusual clinical presentation of intracranial hypertension (IH) and bilateral papilledema. The patient presented with symptoms of increased intracranial pressure, which followed a relapsing, remitting course over several months. Serial CSF studies showed an increased opening pressure during clinical relapses. The CSF and serum tested positive for MOG immunoglobulin G antibodies. Contrast-enhanced MRI of the brain showed mild meningeal enhancement in the left parietal region with subtle underlying cortical hyperintensities, indicating possible fluid-attenuated inversion recovery variable unilateral enhancement of the leptomeninges. The patient responded well to immunosuppressive therapy using rituximab. The presentation of MOG antibody-associated disease (MOGAD) as IH without optic neuritis is rare. This report presents the first description of a relapsing remitting course presenting each time with only symptoms of raised intracranial pressure, without developing any typical clinical manifestations of MOGAD.</p>\",\"PeriodicalId\":520720,\"journal\":{\"name\":\"Neurology(R) neuroimmunology & neuroinflammation\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":7.5000,\"publicationDate\":\"2022-10-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/7f/3f/NXI-2022-200026.PMC9581460.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurology(R) neuroimmunology & neuroinflammation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1212/NXI.0000000000200020\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/11/1 0:00:00\",\"PubModel\":\"Print\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurology(R) neuroimmunology & neuroinflammation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1212/NXI.0000000000200020","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/11/1 0:00:00","PubModel":"Print","JCR":"","JCRName":"","Score":null,"Total":0}
Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease Presenting as Intracranial Hypertension: A Case Report.
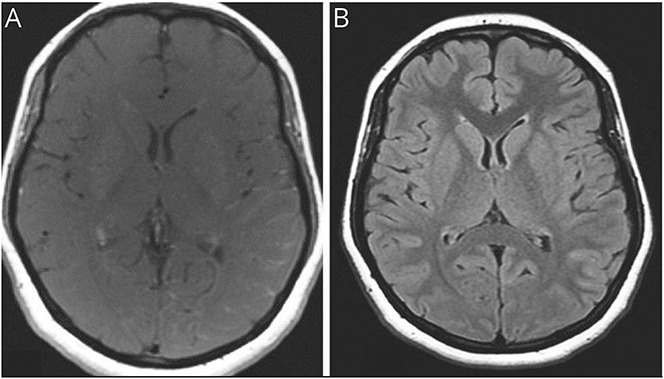
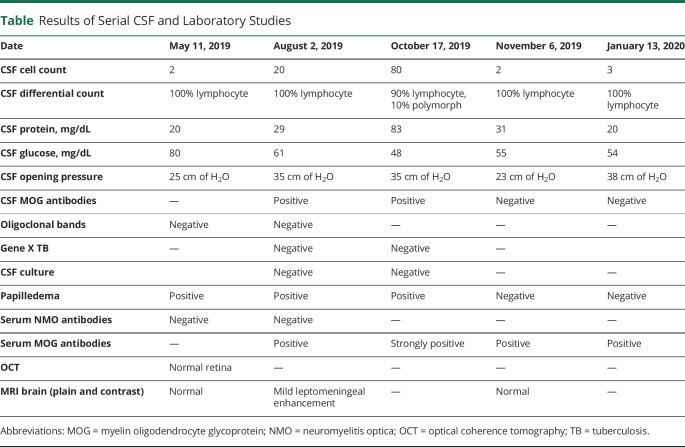
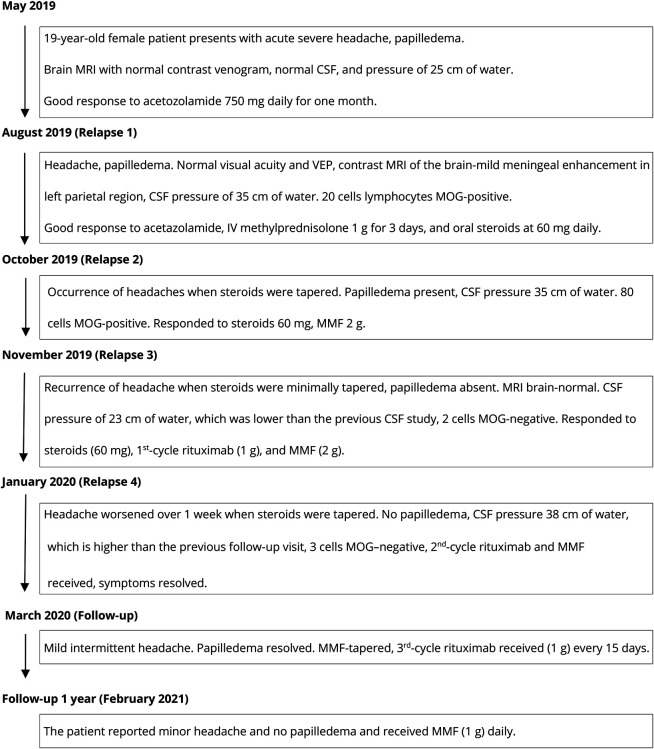
The production of autoantibodies against myelin oligodendrocyte glycoprotein (MOG) can cause a spectrum of autoimmune disorders, including optic neuritis, transverse myelitis, brainstem encephalitis, and acute disseminated encephalomyelitis. In this study, we present the case of a 19-year-old woman with an unusual clinical presentation of intracranial hypertension (IH) and bilateral papilledema. The patient presented with symptoms of increased intracranial pressure, which followed a relapsing, remitting course over several months. Serial CSF studies showed an increased opening pressure during clinical relapses. The CSF and serum tested positive for MOG immunoglobulin G antibodies. Contrast-enhanced MRI of the brain showed mild meningeal enhancement in the left parietal region with subtle underlying cortical hyperintensities, indicating possible fluid-attenuated inversion recovery variable unilateral enhancement of the leptomeninges. The patient responded well to immunosuppressive therapy using rituximab. The presentation of MOG antibody-associated disease (MOGAD) as IH without optic neuritis is rare. This report presents the first description of a relapsing remitting course presenting each time with only symptoms of raised intracranial pressure, without developing any typical clinical manifestations of MOGAD.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


