Massimo A Padalino, Luca Vedovelli, Manuela Simonato, Andrea Bandini, Greta Paganini, Laura Mezzalira, Nicola Faganello, Cristiana Carollo, Dario Gregori, Vladimiro Vida, Paola Cogo
{"title":"先天性心脏病手术患儿体外循环期间保护性持续通气策略的前瞻性研究","authors":"Massimo A Padalino, Luca Vedovelli, Manuela Simonato, Andrea Bandini, Greta Paganini, Laura Mezzalira, Nicola Faganello, Cristiana Carollo, Dario Gregori, Vladimiro Vida, Paola Cogo","doi":"10.1093/icvts/ivac084","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The aim of this study was to evaluate if a 'protective' (low-tidal/low-frequency) ventilation strategy can shorten the postoperative ventilation time and minimize acute lung injury in children with congenital heart disease (CHD) undergoing repair with cardiopulmonary bypass (CPB).</p><p><strong>Methods: </strong>This is a single-centre prospective, interventional study, including children with CHD under the age of 5 years, undergoing open-heart surgery with a CPB >60 min, in hypothermia, haemodynamically stable, and without evident genetic abnormalities. Assist-control ventilation (tidal volume of 4 ml/kg, 10 breaths/min, positive end-expiratory pressure 5 cmH2O and FiO2 0.21) was applied in a cohort of patients during CPB. We compared clinical outcomes and in fully ventilated versus non-ventilated (control) patients. Propensity score was used to weigh ventilated and control groups to correct for the effect of other confounding clinical variables. Clinical and ventilation parameters and lung inflammatory biomarkers in tracheal aspirates were measured. The primary outcome was the postoperative intubation time of more or less than 48 h.</p><p><strong>Results: </strong>We included 140 children (53 ventilated, 87 non-ventilated) with different CHD. There were no deaths or adverse events in ventilated patients. Using a weighted generalized linear model, we found no sufficient evidence for an effect of intraoperative ventilation on postoperative intubation time [estimate 0.13 (95% confidence interval, -0.08; 0.35), P = 0.22].</p><p><strong>Conclusions: </strong>Continuous low-tidal/low-frequency mechanical ventilation during CPB is safe and harmless. However, no significant advantages were found when compared to non-ventilated patients in terms of postoperative ventilation time.</p>","PeriodicalId":13621,"journal":{"name":"Interactive cardiovascular and thoracic surgery","volume":" ","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2022-07-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9297524/pdf/","citationCount":"1","resultStr":"{\"title\":\"Protective continuous ventilation strategy during cardiopulmonary bypass in children undergoing surgery for congenital heart disease: a prospective study.\",\"authors\":\"Massimo A Padalino, Luca Vedovelli, Manuela Simonato, Andrea Bandini, Greta Paganini, Laura Mezzalira, Nicola Faganello, Cristiana Carollo, Dario Gregori, Vladimiro Vida, Paola Cogo\",\"doi\":\"10.1093/icvts/ivac084\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>The aim of this study was to evaluate if a 'protective' (low-tidal/low-frequency) ventilation strategy can shorten the postoperative ventilation time and minimize acute lung injury in children with congenital heart disease (CHD) undergoing repair with cardiopulmonary bypass (CPB).</p><p><strong>Methods: </strong>This is a single-centre prospective, interventional study, including children with CHD under the age of 5 years, undergoing open-heart surgery with a CPB >60 min, in hypothermia, haemodynamically stable, and without evident genetic abnormalities. Assist-control ventilation (tidal volume of 4 ml/kg, 10 breaths/min, positive end-expiratory pressure 5 cmH2O and FiO2 0.21) was applied in a cohort of patients during CPB. We compared clinical outcomes and in fully ventilated versus non-ventilated (control) patients. Propensity score was used to weigh ventilated and control groups to correct for the effect of other confounding clinical variables. Clinical and ventilation parameters and lung inflammatory biomarkers in tracheal aspirates were measured. The primary outcome was the postoperative intubation time of more or less than 48 h.</p><p><strong>Results: </strong>We included 140 children (53 ventilated, 87 non-ventilated) with different CHD. There were no deaths or adverse events in ventilated patients. Using a weighted generalized linear model, we found no sufficient evidence for an effect of intraoperative ventilation on postoperative intubation time [estimate 0.13 (95% confidence interval, -0.08; 0.35), P = 0.22].</p><p><strong>Conclusions: </strong>Continuous low-tidal/low-frequency mechanical ventilation during CPB is safe and harmless. However, no significant advantages were found when compared to non-ventilated patients in terms of postoperative ventilation time.</p>\",\"PeriodicalId\":13621,\"journal\":{\"name\":\"Interactive cardiovascular and thoracic surgery\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2022-07-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9297524/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Interactive cardiovascular and thoracic surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/icvts/ivac084\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interactive cardiovascular and thoracic surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/icvts/ivac084","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 1
摘要
目的:本研究的目的是评估“保护性”(低潮/低频)通气策略是否可以缩短先天性心脏病(CHD)患儿行体外循环修复术(CPB)的术后通气时间并最大限度地减少急性肺损伤。方法:这是一项单中心前瞻性干预性研究,包括5岁以下的CHD儿童,接受体外循环>60分钟的心内直视手术,体温过低,血流动力学稳定,无明显遗传异常。辅助控制通气(潮气量4 ml/kg, 10次呼吸/min,呼气末正压5 cmH2O和FiO2 0.21)应用于CPB期间的患者队列。我们比较了完全通气与非通气(对照)患者的临床结果。倾向评分用于权衡通气组和对照组,以纠正其他混杂临床变量的影响。测量气管吸入者的临床和通气参数以及肺部炎症生物标志物。主要观察指标为术后插管时间≥48 h。结果:纳入140例不同冠心病患儿(53例通气患儿,87例非通气患儿)。通气患者无死亡或不良事件发生。使用加权广义线性模型,我们没有发现足够的证据表明术中通气对术后插管时间的影响[估计0.13(95%可信区间,-0.08;0.35), p = 0.22]。结论:CPB期间持续低潮/低频机械通气是安全无害的。然而,与非通气患者相比,术后通气时间没有明显优势。
Protective continuous ventilation strategy during cardiopulmonary bypass in children undergoing surgery for congenital heart disease: a prospective study.
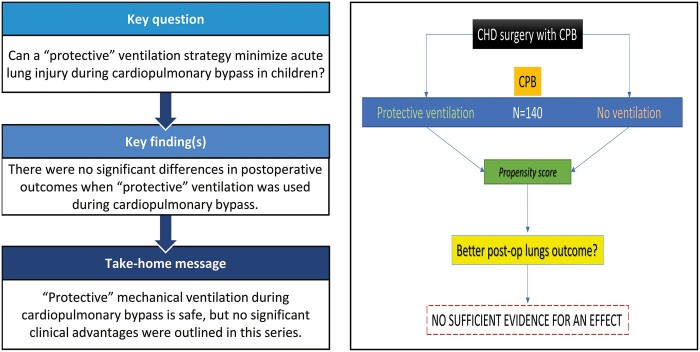
Objectives: The aim of this study was to evaluate if a 'protective' (low-tidal/low-frequency) ventilation strategy can shorten the postoperative ventilation time and minimize acute lung injury in children with congenital heart disease (CHD) undergoing repair with cardiopulmonary bypass (CPB).
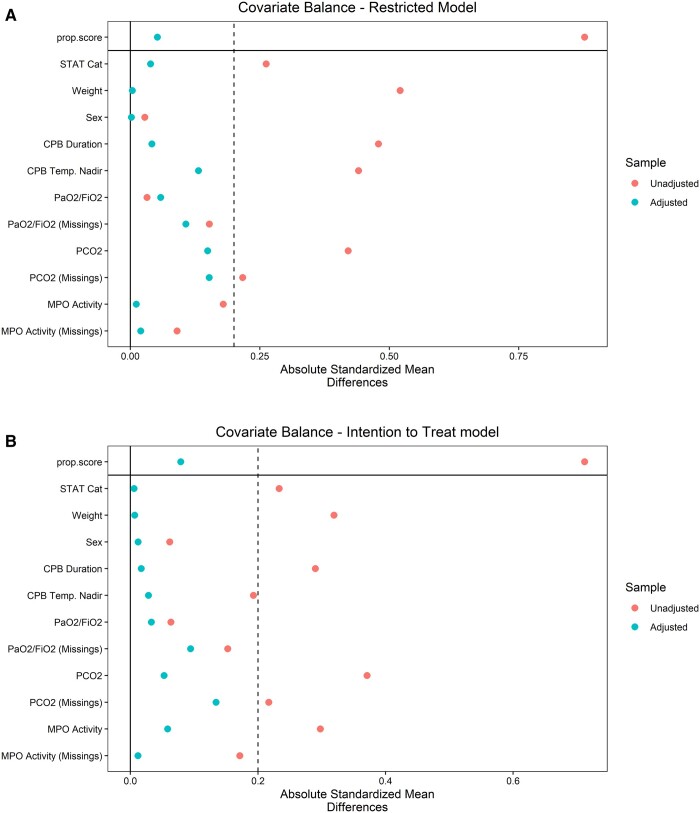
Methods: This is a single-centre prospective, interventional study, including children with CHD under the age of 5 years, undergoing open-heart surgery with a CPB >60 min, in hypothermia, haemodynamically stable, and without evident genetic abnormalities. Assist-control ventilation (tidal volume of 4 ml/kg, 10 breaths/min, positive end-expiratory pressure 5 cmH2O and FiO2 0.21) was applied in a cohort of patients during CPB. We compared clinical outcomes and in fully ventilated versus non-ventilated (control) patients. Propensity score was used to weigh ventilated and control groups to correct for the effect of other confounding clinical variables. Clinical and ventilation parameters and lung inflammatory biomarkers in tracheal aspirates were measured. The primary outcome was the postoperative intubation time of more or less than 48 h.
Results: We included 140 children (53 ventilated, 87 non-ventilated) with different CHD. There were no deaths or adverse events in ventilated patients. Using a weighted generalized linear model, we found no sufficient evidence for an effect of intraoperative ventilation on postoperative intubation time [estimate 0.13 (95% confidence interval, -0.08; 0.35), P = 0.22].
Conclusions: Continuous low-tidal/low-frequency mechanical ventilation during CPB is safe and harmless. However, no significant advantages were found when compared to non-ventilated patients in terms of postoperative ventilation time.
期刊介绍:
Interactive CardioVascular and Thoracic Surgery (ICVTS) publishes scientific contributions in the field of cardiovascular and thoracic surgery, covering all aspects of surgery of the heart, vessels and the chest. The journal publishes a range of article types including: Best Evidence Topics; Brief Communications; Case Reports; Original Articles; State-of-the-Art; Work in Progress Report.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


