{"title":"非囊性纤维化支气管扩张患者肺弥散能力受损的相关危险因素","authors":"Kaijun Zhang, Xin Zou, Zhiyi Ma, Xiaohong Liu, Chencheng Qiu, Lingyan Xie, Zhaosheng Lin, Saiyu Li, Yongming Wu","doi":"10.1155/2022/8175508","DOIUrl":null,"url":null,"abstract":"<p><p>This study aims to investigate the risk factors associated with impaired pulmonary diffusing capacity among patients with noncystic fibrosis bronchiectasis (NCFB) and compare the predictive value of several scoring systems for the impairment in these patients. Between July 2019 and June 2021, patients who were admitted to the hospital and diagnosed with NCFB were included in this study. Clinical data were collected and analyzed retrospectively. A total of 175 NCFB patients were included in the analysis. Multivariate logistic regression analysis revealed that impaired pulmonary diffusing capacity diagnosed by carbon monoxide diffusing capacity (DLCO) <80% prediction was associated with age, Reiff score, body mass index (BMI), comorbid chronic obstructive pulmonary disease (COPD), and interstitial lung disease (ILD). Disease duration, frequency of exacerbation, hemoglobin level, and COPD were independent risk factors for impaired pulmonary diffusing capacity diagnosed by DLCO/alveolar volume (VA) <80% prediction. Age, Reiff score, and smoking status were independent risk factors for decreased VA diagnosed by VA <80% prediction. The areas under the curve (AUC) for discrimination of DLCO <80% prediction were 0.822 (0.760-0.885) for Bronchiectasis Severity Index (BSI), 0.787 (0.718-0.856) for FACED, 0.795 (0.729-0.863) for E-FACED, and 0.767 (0.694-0.839) for modified Medical Research Council (mMRC) scores; the AUC for discrimination of DLCO/VA <80% prediction was 0.803 (0.727-0.880) for BSI, 0.752 (0.669-0.835) for FACED, 0.757 (0.676-0.839) for E-FACED, and 0.762 (0.679-0.845) for mMRC, respectively. The BSI had the largest AUC, but the differences between those scoring systems had no statistical significance (<i>P</i>=0.181 for DLCO <80% prediction and <i>P</i>=0.105 for DLCO/VA <80% prediction). The mMRC score (up to 2 grades) showed a high specificity for discriminating diffusing dysfunction (88.3% for DLCO <80% prediction and 76.1% for DLCO/VA <80% prediction). In NCFB patients, several factors such as age, Reiff score, BMI, exacerbation frequency, disease duration, and comorbid COPD and ILD were associated with impaired pulmonary diffusing capacity, which requires more attention in managing those patients. In addition, several scoring methods, including a simple index of mMRC, showed a comparable and moderate performance for predicting pulmonary diffusing impairment and would facilitate the systematic evaluation of the diffusing capacity of NCFB patients.</p>","PeriodicalId":9416,"journal":{"name":"Canadian respiratory journal","volume":null,"pages":null},"PeriodicalIF":2.1000,"publicationDate":"2022-03-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8926517/pdf/","citationCount":"1","resultStr":"{\"title\":\"Risk Factors Associated with Impairment in Pulmonary Diffusing Capacity among Patients with Noncystic Fibrosis Bronchiectasis.\",\"authors\":\"Kaijun Zhang, Xin Zou, Zhiyi Ma, Xiaohong Liu, Chencheng Qiu, Lingyan Xie, Zhaosheng Lin, Saiyu Li, Yongming Wu\",\"doi\":\"10.1155/2022/8175508\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>This study aims to investigate the risk factors associated with impaired pulmonary diffusing capacity among patients with noncystic fibrosis bronchiectasis (NCFB) and compare the predictive value of several scoring systems for the impairment in these patients. Between July 2019 and June 2021, patients who were admitted to the hospital and diagnosed with NCFB were included in this study. Clinical data were collected and analyzed retrospectively. A total of 175 NCFB patients were included in the analysis. Multivariate logistic regression analysis revealed that impaired pulmonary diffusing capacity diagnosed by carbon monoxide diffusing capacity (DLCO) <80% prediction was associated with age, Reiff score, body mass index (BMI), comorbid chronic obstructive pulmonary disease (COPD), and interstitial lung disease (ILD). Disease duration, frequency of exacerbation, hemoglobin level, and COPD were independent risk factors for impaired pulmonary diffusing capacity diagnosed by DLCO/alveolar volume (VA) <80% prediction. Age, Reiff score, and smoking status were independent risk factors for decreased VA diagnosed by VA <80% prediction. The areas under the curve (AUC) for discrimination of DLCO <80% prediction were 0.822 (0.760-0.885) for Bronchiectasis Severity Index (BSI), 0.787 (0.718-0.856) for FACED, 0.795 (0.729-0.863) for E-FACED, and 0.767 (0.694-0.839) for modified Medical Research Council (mMRC) scores; the AUC for discrimination of DLCO/VA <80% prediction was 0.803 (0.727-0.880) for BSI, 0.752 (0.669-0.835) for FACED, 0.757 (0.676-0.839) for E-FACED, and 0.762 (0.679-0.845) for mMRC, respectively. The BSI had the largest AUC, but the differences between those scoring systems had no statistical significance (<i>P</i>=0.181 for DLCO <80% prediction and <i>P</i>=0.105 for DLCO/VA <80% prediction). The mMRC score (up to 2 grades) showed a high specificity for discriminating diffusing dysfunction (88.3% for DLCO <80% prediction and 76.1% for DLCO/VA <80% prediction). In NCFB patients, several factors such as age, Reiff score, BMI, exacerbation frequency, disease duration, and comorbid COPD and ILD were associated with impaired pulmonary diffusing capacity, which requires more attention in managing those patients. In addition, several scoring methods, including a simple index of mMRC, showed a comparable and moderate performance for predicting pulmonary diffusing impairment and would facilitate the systematic evaluation of the diffusing capacity of NCFB patients.</p>\",\"PeriodicalId\":9416,\"journal\":{\"name\":\"Canadian respiratory journal\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2022-03-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8926517/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Canadian respiratory journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1155/2022/8175508\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian respiratory journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/2022/8175508","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
Risk Factors Associated with Impairment in Pulmonary Diffusing Capacity among Patients with Noncystic Fibrosis Bronchiectasis.
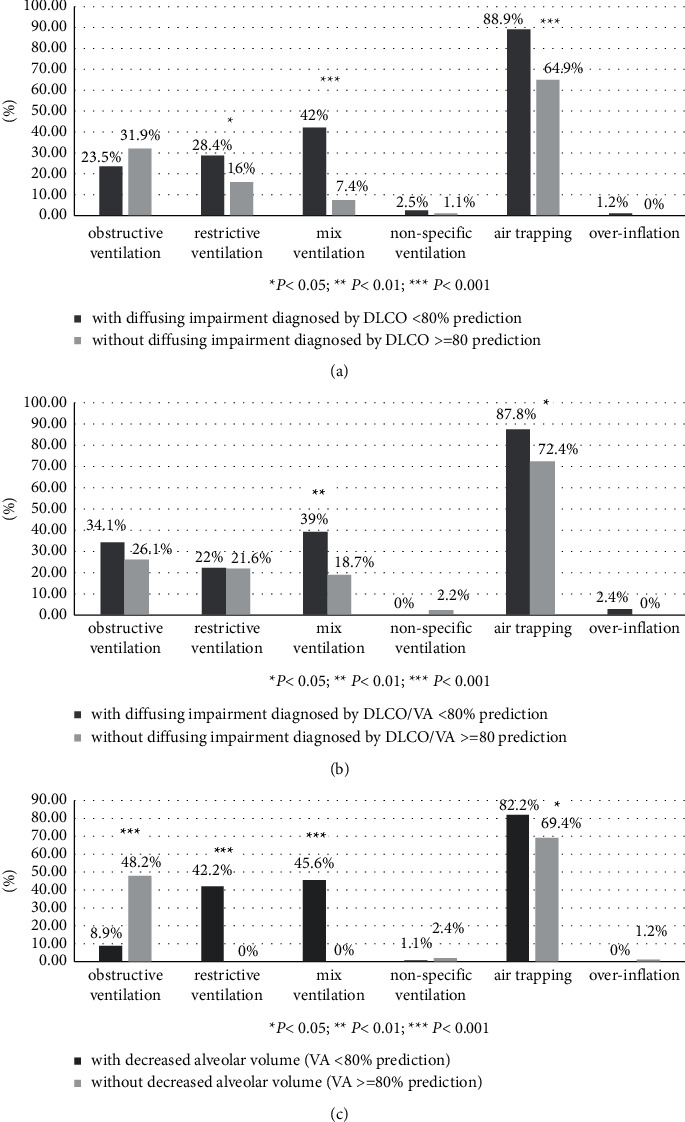
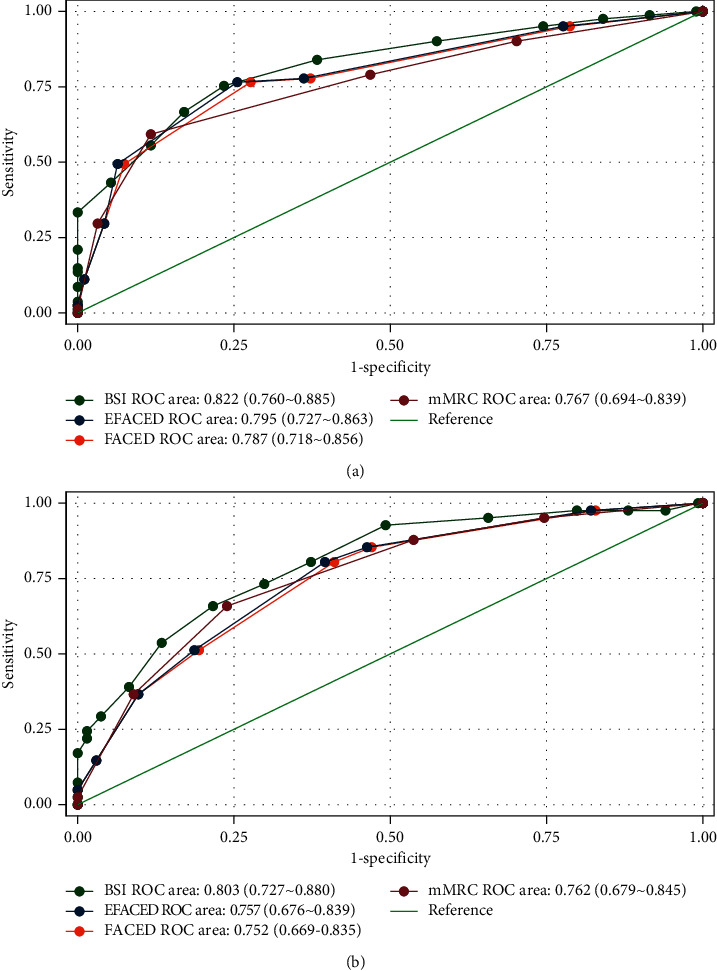
This study aims to investigate the risk factors associated with impaired pulmonary diffusing capacity among patients with noncystic fibrosis bronchiectasis (NCFB) and compare the predictive value of several scoring systems for the impairment in these patients. Between July 2019 and June 2021, patients who were admitted to the hospital and diagnosed with NCFB were included in this study. Clinical data were collected and analyzed retrospectively. A total of 175 NCFB patients were included in the analysis. Multivariate logistic regression analysis revealed that impaired pulmonary diffusing capacity diagnosed by carbon monoxide diffusing capacity (DLCO) <80% prediction was associated with age, Reiff score, body mass index (BMI), comorbid chronic obstructive pulmonary disease (COPD), and interstitial lung disease (ILD). Disease duration, frequency of exacerbation, hemoglobin level, and COPD were independent risk factors for impaired pulmonary diffusing capacity diagnosed by DLCO/alveolar volume (VA) <80% prediction. Age, Reiff score, and smoking status were independent risk factors for decreased VA diagnosed by VA <80% prediction. The areas under the curve (AUC) for discrimination of DLCO <80% prediction were 0.822 (0.760-0.885) for Bronchiectasis Severity Index (BSI), 0.787 (0.718-0.856) for FACED, 0.795 (0.729-0.863) for E-FACED, and 0.767 (0.694-0.839) for modified Medical Research Council (mMRC) scores; the AUC for discrimination of DLCO/VA <80% prediction was 0.803 (0.727-0.880) for BSI, 0.752 (0.669-0.835) for FACED, 0.757 (0.676-0.839) for E-FACED, and 0.762 (0.679-0.845) for mMRC, respectively. The BSI had the largest AUC, but the differences between those scoring systems had no statistical significance (P=0.181 for DLCO <80% prediction and P=0.105 for DLCO/VA <80% prediction). The mMRC score (up to 2 grades) showed a high specificity for discriminating diffusing dysfunction (88.3% for DLCO <80% prediction and 76.1% for DLCO/VA <80% prediction). In NCFB patients, several factors such as age, Reiff score, BMI, exacerbation frequency, disease duration, and comorbid COPD and ILD were associated with impaired pulmonary diffusing capacity, which requires more attention in managing those patients. In addition, several scoring methods, including a simple index of mMRC, showed a comparable and moderate performance for predicting pulmonary diffusing impairment and would facilitate the systematic evaluation of the diffusing capacity of NCFB patients.
期刊介绍:
Canadian Respiratory Journal is a peer-reviewed, Open Access journal that aims to provide a multidisciplinary forum for research in all areas of respiratory medicine. The journal publishes original research articles, review articles, and clinical studies related to asthma, allergy, COPD, non-invasive ventilation, therapeutic intervention, lung cancer, airway and lung infections, as well as any other respiratory diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


