{"title":"中性粒细胞减少患者食管肺肺病的偶然发现。","authors":"Seung-Ah Yahng, Hee-Je Kim","doi":"10.5045/kjh.2011.46.3.151","DOIUrl":null,"url":null,"abstract":"which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. A 62-year-old woman with relapsed acute myeloid leukemia occurring 181 days after autologous stem-cell transplantation underwent reinduction chemotherapy as per the FLANG regimen (fludarabine 30 mg/m 2 /day, cytosine arabinoside 1 g/m 2 /day, mitoxantrone 10 mg/m 2 /day, and granulocyte colony-stimulating factor 300 μg/day for 5 days). On post-chemotherapy day 5, neutropenic fever developed and empirical antibiotic therapy was prescribed. Chest radiography performed 3 days later revealed several patchy consolidations on both lung fields. Physical examination yielded unremarkable results, except mild oral mucositis. Serum galactomannan assay was elevated (>6.4). Chest computed tomography (CT) showed multifocal, patchy consolidations with surrounding ground-glass opacities in both lung parenchyma and infiltration along the bronchial trees (A). Further, we detected esophageal wall thickening with intramuscular air bubbles in the upper esophagus but sparing gastric and lower intestinal walls, indicating esophageal pneumatosis (B, C arrow). Since the patient reported no associated symptoms, no active treatment was considered other than total parenteral nutrition while amphoteric was added. Follow-up chest CT 14 days later revealed regression of pneumatosis but progression of pneumonia with cavity formation. Despite intensive management with daily donor granulocyte transfusions and mechanical ventilation, the patient died of progressive acute respiratory distress syndrome on post-chemotherapy day 43.","PeriodicalId":23001,"journal":{"name":"The Korean Journal of Hematology","volume":"46 3","pages":"151"},"PeriodicalIF":0.0000,"publicationDate":"2011-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.5045/kjh.2011.46.3.151","citationCount":"4","resultStr":"{\"title\":\"Fortuitous detection of esophageal pneumatosis in a neutropenic patient.\",\"authors\":\"Seung-Ah Yahng, Hee-Je Kim\",\"doi\":\"10.5045/kjh.2011.46.3.151\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. A 62-year-old woman with relapsed acute myeloid leukemia occurring 181 days after autologous stem-cell transplantation underwent reinduction chemotherapy as per the FLANG regimen (fludarabine 30 mg/m 2 /day, cytosine arabinoside 1 g/m 2 /day, mitoxantrone 10 mg/m 2 /day, and granulocyte colony-stimulating factor 300 μg/day for 5 days). On post-chemotherapy day 5, neutropenic fever developed and empirical antibiotic therapy was prescribed. Chest radiography performed 3 days later revealed several patchy consolidations on both lung fields. Physical examination yielded unremarkable results, except mild oral mucositis. Serum galactomannan assay was elevated (>6.4). Chest computed tomography (CT) showed multifocal, patchy consolidations with surrounding ground-glass opacities in both lung parenchyma and infiltration along the bronchial trees (A). Further, we detected esophageal wall thickening with intramuscular air bubbles in the upper esophagus but sparing gastric and lower intestinal walls, indicating esophageal pneumatosis (B, C arrow). Since the patient reported no associated symptoms, no active treatment was considered other than total parenteral nutrition while amphoteric was added. Follow-up chest CT 14 days later revealed regression of pneumatosis but progression of pneumonia with cavity formation. Despite intensive management with daily donor granulocyte transfusions and mechanical ventilation, the patient died of progressive acute respiratory distress syndrome on post-chemotherapy day 43.\",\"PeriodicalId\":23001,\"journal\":{\"name\":\"The Korean Journal of Hematology\",\"volume\":\"46 3\",\"pages\":\"151\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2011-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.5045/kjh.2011.46.3.151\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Korean Journal of Hematology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5045/kjh.2011.46.3.151\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2011/9/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Korean Journal of Hematology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5045/kjh.2011.46.3.151","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2011/9/30 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Fortuitous detection of esophageal pneumatosis in a neutropenic patient.
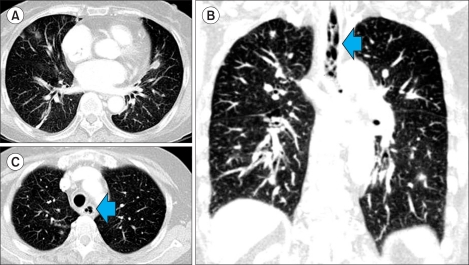
which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. A 62-year-old woman with relapsed acute myeloid leukemia occurring 181 days after autologous stem-cell transplantation underwent reinduction chemotherapy as per the FLANG regimen (fludarabine 30 mg/m 2 /day, cytosine arabinoside 1 g/m 2 /day, mitoxantrone 10 mg/m 2 /day, and granulocyte colony-stimulating factor 300 μg/day for 5 days). On post-chemotherapy day 5, neutropenic fever developed and empirical antibiotic therapy was prescribed. Chest radiography performed 3 days later revealed several patchy consolidations on both lung fields. Physical examination yielded unremarkable results, except mild oral mucositis. Serum galactomannan assay was elevated (>6.4). Chest computed tomography (CT) showed multifocal, patchy consolidations with surrounding ground-glass opacities in both lung parenchyma and infiltration along the bronchial trees (A). Further, we detected esophageal wall thickening with intramuscular air bubbles in the upper esophagus but sparing gastric and lower intestinal walls, indicating esophageal pneumatosis (B, C arrow). Since the patient reported no associated symptoms, no active treatment was considered other than total parenteral nutrition while amphoteric was added. Follow-up chest CT 14 days later revealed regression of pneumatosis but progression of pneumonia with cavity formation. Despite intensive management with daily donor granulocyte transfusions and mechanical ventilation, the patient died of progressive acute respiratory distress syndrome on post-chemotherapy day 43.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


