Tara Gomes, David N Juurlink, Irfan A Dhalla, Angela Mailis-Gagnon, J Michael Paterson, Muhammad M Mamdani
{"title":"社会经济弱势患者阿片类药物使用和给药趋势。","authors":"Tara Gomes, David N Juurlink, Irfan A Dhalla, Angela Mailis-Gagnon, J Michael Paterson, Muhammad M Mamdani","doi":"","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Opioid therapy for patients with chronic nonmalignant pain remains controversial, primarily because of safety concerns and the potential for abuse. The objective of this study was to examine trends in opioid utilization for nonmalignant pain among recipients of social assistance and to explore the relation between dose of analgesic and mortality.</p><p><strong>Methods: </strong>Using a cross-sectional study design, we characterized annual trends in prescriptions for and daily dose of opioid analgesics between 2003 and 2008 for beneficiaries (aged 15 to 64 years) of Ontario's public drug plan. We defined moderate, high and very high dose thresholds as daily doses of up to 200, 201 to 400, and more than 400 mg oral morphine (or equivalent), respectively. In an exploratory cohort study, we followed, over a 2-year period, patients who received at least one prescription for an opioid in 2004 to investigate the relation between opioid dose and opioid-related mortality.</p><p><strong>Results: </strong>Over the study period, opioid prescribing rates rose by 16.2%, and 180 974 individuals received nearly 1.5 million opioid prescriptions in 2008. Also by 2008, the daily dose dispensed exceeded 200 mg morphine equivalent for almost a third (32.6%) of recipients of long-acting oxycodone but only 20.3% of those treated with fentanyl or other long-acting opioids. Among patients for whom high or very high doses of opioids were dispensed in 2004, 19.3% of deaths during the subsequent 2 years were opioid-related, occurring at a median age of 46 years. Two-year opioid-related mortality rates were 1.63 per 1000 population (95% confidence interval [CI] 1.42-1.85) among people with moderate-dose prescriptions, 7.92 per 1000 population (95% CI 5.25-11.49) among those with high-dose prescriptions, and 9.94 per 1000 population (95% CI 2.78-25.12) among those with very-high-dose prescriptions.</p><p><strong>Interpretation: </strong>Among socio-economically disadvantaged patients in Ontario, the use and dose of opioids for nonmalignant pain has increased substantially, driven primarily by the use of long-acting oxycodone and, to a lesser extent, fentanyl. The findings of our exploratory study suggested a strong association between opioid-related mortality and the dose of opioid dispensed.</p>","PeriodicalId":88624,"journal":{"name":"Open medicine : a peer-reviewed, independent, open-access journal","volume":"5 1","pages":"e13-22"},"PeriodicalIF":0.0000,"publicationDate":"2011-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ad/85/OpenMed-05-e13.PMC3205807.pdf","citationCount":"0","resultStr":"{\"title\":\"Trends in opioid use and dosing among socio-economically disadvantaged patients.\",\"authors\":\"Tara Gomes, David N Juurlink, Irfan A Dhalla, Angela Mailis-Gagnon, J Michael Paterson, Muhammad M Mamdani\",\"doi\":\"\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Opioid therapy for patients with chronic nonmalignant pain remains controversial, primarily because of safety concerns and the potential for abuse. The objective of this study was to examine trends in opioid utilization for nonmalignant pain among recipients of social assistance and to explore the relation between dose of analgesic and mortality.</p><p><strong>Methods: </strong>Using a cross-sectional study design, we characterized annual trends in prescriptions for and daily dose of opioid analgesics between 2003 and 2008 for beneficiaries (aged 15 to 64 years) of Ontario's public drug plan. We defined moderate, high and very high dose thresholds as daily doses of up to 200, 201 to 400, and more than 400 mg oral morphine (or equivalent), respectively. In an exploratory cohort study, we followed, over a 2-year period, patients who received at least one prescription for an opioid in 2004 to investigate the relation between opioid dose and opioid-related mortality.</p><p><strong>Results: </strong>Over the study period, opioid prescribing rates rose by 16.2%, and 180 974 individuals received nearly 1.5 million opioid prescriptions in 2008. Also by 2008, the daily dose dispensed exceeded 200 mg morphine equivalent for almost a third (32.6%) of recipients of long-acting oxycodone but only 20.3% of those treated with fentanyl or other long-acting opioids. Among patients for whom high or very high doses of opioids were dispensed in 2004, 19.3% of deaths during the subsequent 2 years were opioid-related, occurring at a median age of 46 years. Two-year opioid-related mortality rates were 1.63 per 1000 population (95% confidence interval [CI] 1.42-1.85) among people with moderate-dose prescriptions, 7.92 per 1000 population (95% CI 5.25-11.49) among those with high-dose prescriptions, and 9.94 per 1000 population (95% CI 2.78-25.12) among those with very-high-dose prescriptions.</p><p><strong>Interpretation: </strong>Among socio-economically disadvantaged patients in Ontario, the use and dose of opioids for nonmalignant pain has increased substantially, driven primarily by the use of long-acting oxycodone and, to a lesser extent, fentanyl. The findings of our exploratory study suggested a strong association between opioid-related mortality and the dose of opioid dispensed.</p>\",\"PeriodicalId\":88624,\"journal\":{\"name\":\"Open medicine : a peer-reviewed, independent, open-access journal\",\"volume\":\"5 1\",\"pages\":\"e13-22\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2011-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ad/85/OpenMed-05-e13.PMC3205807.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open medicine : a peer-reviewed, independent, open-access journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2011/1/25 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open medicine : a peer-reviewed, independent, open-access journal","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2011/1/25 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:阿片类药物治疗慢性非恶性疼痛患者仍然存在争议,主要是因为安全性问题和滥用的可能性。本研究的目的是研究阿片类药物在社会救助接受者中用于治疗非恶性疼痛的趋势,并探讨止痛药剂量与死亡率之间的关系。方法:采用横断面研究设计,我们描述了2003年至2008年安大略省公共药物计划受益人(15至64岁)阿片类镇痛药处方和日剂量的年度趋势。我们将中度、高剂量和极高剂量阈值分别定义为每日口服吗啡剂量高达200mg、201至400mg和超过400mg(或同等剂量)。在一项探索性队列研究中,我们对2004年至少接受过一次阿片类药物处方的患者进行了为期2年的随访,以调查阿片类药物剂量与阿片类药物相关死亡率之间的关系。结果:在研究期间,阿片类药物处方率上升了16.2%,2008年有180974人获得了近150万张阿片类药物处方。同样,到2008年,近三分之一(32.6%)长效羟考酮接受者的日剂量超过200毫克吗啡当量,而芬太尼或其他长效阿片类药物接受者的日剂量仅为20.3%。在2004年使用高剂量或非常高剂量阿片类药物的患者中,在随后的2年中,19.3%的死亡与阿片类药物有关,发生的中位年龄为46岁。在中等剂量处方人群中,两年阿片类药物相关死亡率为1.63 / 1000(95%可信区间[CI] 1.42-1.85),在高剂量处方人群中为7.92 / 1000 (95% CI 5.25-11.49),在高剂量处方人群中为9.94 / 1000 (95% CI 2.78-25.12)。解释:在安大略省社会经济条件较差的患者中,阿片类药物治疗非恶性疼痛的使用和剂量大幅增加,主要是由于长效羟考酮的使用,芬太尼的使用程度较低。我们的探索性研究结果表明,阿片类药物相关死亡率与阿片类药物的剂量有很强的相关性。
Trends in opioid use and dosing among socio-economically disadvantaged patients.
Background: Opioid therapy for patients with chronic nonmalignant pain remains controversial, primarily because of safety concerns and the potential for abuse. The objective of this study was to examine trends in opioid utilization for nonmalignant pain among recipients of social assistance and to explore the relation between dose of analgesic and mortality.
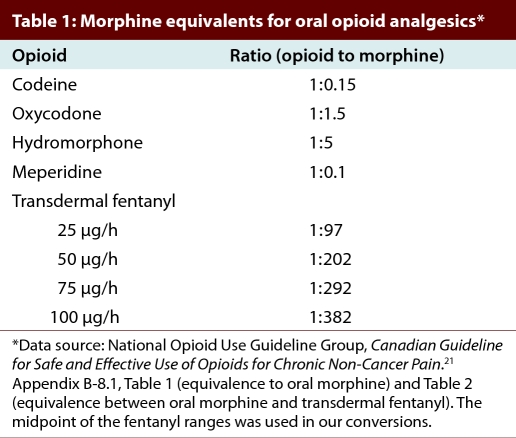
Methods: Using a cross-sectional study design, we characterized annual trends in prescriptions for and daily dose of opioid analgesics between 2003 and 2008 for beneficiaries (aged 15 to 64 years) of Ontario's public drug plan. We defined moderate, high and very high dose thresholds as daily doses of up to 200, 201 to 400, and more than 400 mg oral morphine (or equivalent), respectively. In an exploratory cohort study, we followed, over a 2-year period, patients who received at least one prescription for an opioid in 2004 to investigate the relation between opioid dose and opioid-related mortality.
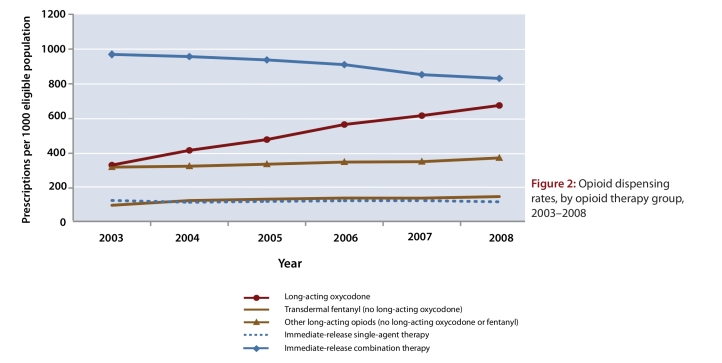
Results: Over the study period, opioid prescribing rates rose by 16.2%, and 180 974 individuals received nearly 1.5 million opioid prescriptions in 2008. Also by 2008, the daily dose dispensed exceeded 200 mg morphine equivalent for almost a third (32.6%) of recipients of long-acting oxycodone but only 20.3% of those treated with fentanyl or other long-acting opioids. Among patients for whom high or very high doses of opioids were dispensed in 2004, 19.3% of deaths during the subsequent 2 years were opioid-related, occurring at a median age of 46 years. Two-year opioid-related mortality rates were 1.63 per 1000 population (95% confidence interval [CI] 1.42-1.85) among people with moderate-dose prescriptions, 7.92 per 1000 population (95% CI 5.25-11.49) among those with high-dose prescriptions, and 9.94 per 1000 population (95% CI 2.78-25.12) among those with very-high-dose prescriptions.
Interpretation: Among socio-economically disadvantaged patients in Ontario, the use and dose of opioids for nonmalignant pain has increased substantially, driven primarily by the use of long-acting oxycodone and, to a lesser extent, fentanyl. The findings of our exploratory study suggested a strong association between opioid-related mortality and the dose of opioid dispensed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


