Thomas Bieganowski, Daniel B Buchalter, Vivek Singh, John J Mercuri, Vinay K Aggarwal, Joshua C Rozell, Ran Schwarzkopf
{"title":"无菌翻修全膝关节置换术中的骨丢失:处理和结果。","authors":"Thomas Bieganowski, Daniel B Buchalter, Vivek Singh, John J Mercuri, Vinay K Aggarwal, Joshua C Rozell, Ran Schwarzkopf","doi":"10.1186/s43019-022-00158-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Although several techniques and implants have been developed to address bone loss in revision total knee arthroplasty (rTKA), management of these defects remains challenging. This review article discusses the indications and management options of bone loss following total knee arthroplasty based on preoperative workup and intraoperative findings.</p><p><strong>Main text: </strong>Various imaging modalities are available that can be augmented with intraoperative examination to provide a clear classification of a bony defect. For this reason, the Anderson Orthopaedic Research Institute (AORI) classification is frequently used to guide treatment. The AORI provides a reliable system by which surgeons can classify lesions based on their size and involvement of surrounding structures. AORI type I defects are managed with cement with or without screws as well as impaction bone grafting. For AORI type IIA lesions, wedge or block augmentation is available. For large defects encompassing AORI type IIB and type III defects, bulk allografts, cones, sleeves, and megaprostheses can be used in conjunction with intramedullary stems.</p><p><strong>Conclusions: </strong>Treatment of bone loss in rTKA continues to evolve as different techniques and approaches have been validated through short- and mid-term follow-up. Extensive preoperative planning with imaging, accurate intraoperative evaluation of the bone loss, and comprehensive understanding of all the implant options available for the bone loss are paramount to success.</p>","PeriodicalId":17886,"journal":{"name":"Knee Surgery & Related Research","volume":" ","pages":"30"},"PeriodicalIF":4.4000,"publicationDate":"2022-06-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9208118/pdf/","citationCount":"4","resultStr":"{\"title\":\"Bone loss in aseptic revision total knee arthroplasty: management and outcomes.\",\"authors\":\"Thomas Bieganowski, Daniel B Buchalter, Vivek Singh, John J Mercuri, Vinay K Aggarwal, Joshua C Rozell, Ran Schwarzkopf\",\"doi\":\"10.1186/s43019-022-00158-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Although several techniques and implants have been developed to address bone loss in revision total knee arthroplasty (rTKA), management of these defects remains challenging. This review article discusses the indications and management options of bone loss following total knee arthroplasty based on preoperative workup and intraoperative findings.</p><p><strong>Main text: </strong>Various imaging modalities are available that can be augmented with intraoperative examination to provide a clear classification of a bony defect. For this reason, the Anderson Orthopaedic Research Institute (AORI) classification is frequently used to guide treatment. The AORI provides a reliable system by which surgeons can classify lesions based on their size and involvement of surrounding structures. AORI type I defects are managed with cement with or without screws as well as impaction bone grafting. For AORI type IIA lesions, wedge or block augmentation is available. For large defects encompassing AORI type IIB and type III defects, bulk allografts, cones, sleeves, and megaprostheses can be used in conjunction with intramedullary stems.</p><p><strong>Conclusions: </strong>Treatment of bone loss in rTKA continues to evolve as different techniques and approaches have been validated through short- and mid-term follow-up. Extensive preoperative planning with imaging, accurate intraoperative evaluation of the bone loss, and comprehensive understanding of all the implant options available for the bone loss are paramount to success.</p>\",\"PeriodicalId\":17886,\"journal\":{\"name\":\"Knee Surgery & Related Research\",\"volume\":\" \",\"pages\":\"30\"},\"PeriodicalIF\":4.4000,\"publicationDate\":\"2022-06-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9208118/pdf/\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Knee Surgery & Related Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s43019-022-00158-y\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Knee Surgery & Related Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s43019-022-00158-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Bone loss in aseptic revision total knee arthroplasty: management and outcomes.
Background: Although several techniques and implants have been developed to address bone loss in revision total knee arthroplasty (rTKA), management of these defects remains challenging. This review article discusses the indications and management options of bone loss following total knee arthroplasty based on preoperative workup and intraoperative findings.
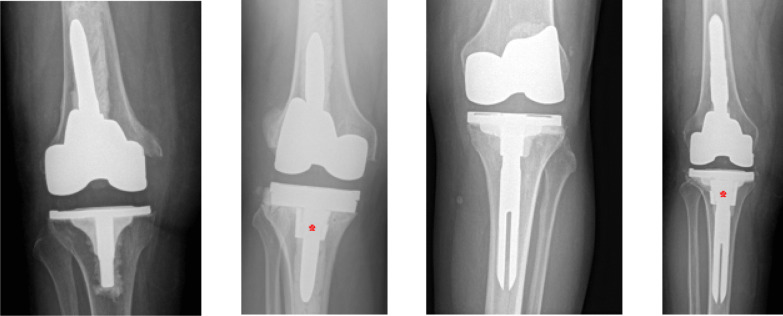
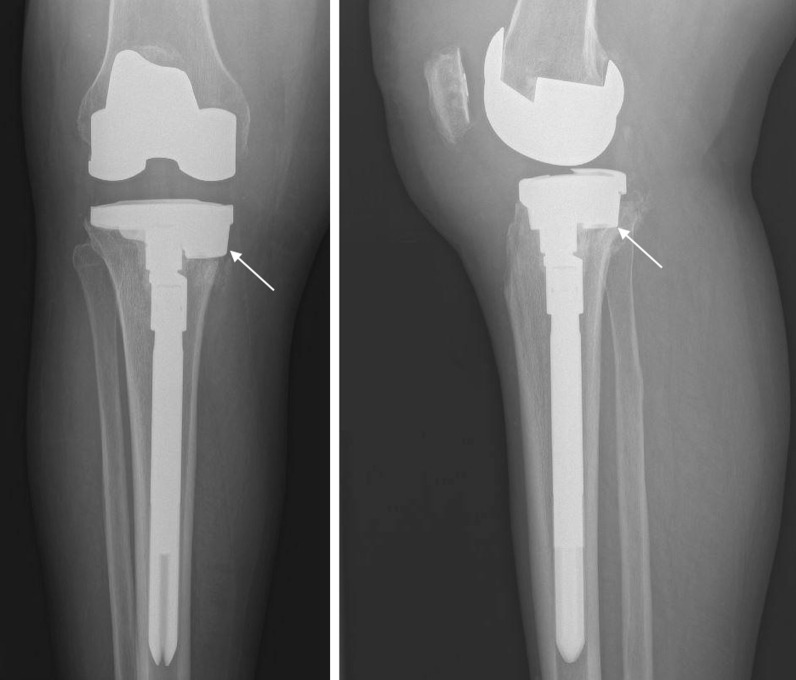
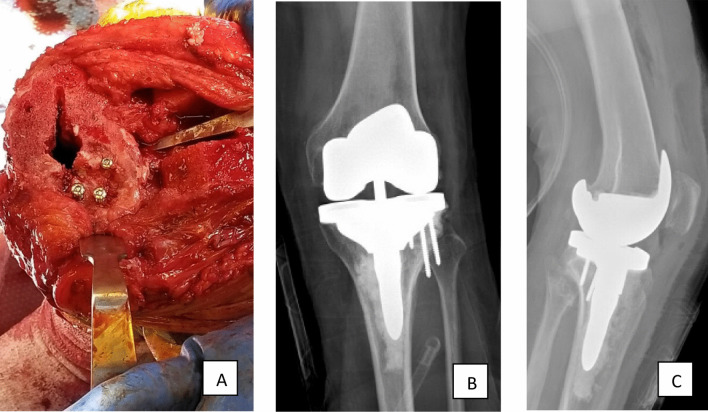
Main text: Various imaging modalities are available that can be augmented with intraoperative examination to provide a clear classification of a bony defect. For this reason, the Anderson Orthopaedic Research Institute (AORI) classification is frequently used to guide treatment. The AORI provides a reliable system by which surgeons can classify lesions based on their size and involvement of surrounding structures. AORI type I defects are managed with cement with or without screws as well as impaction bone grafting. For AORI type IIA lesions, wedge or block augmentation is available. For large defects encompassing AORI type IIB and type III defects, bulk allografts, cones, sleeves, and megaprostheses can be used in conjunction with intramedullary stems.
Conclusions: Treatment of bone loss in rTKA continues to evolve as different techniques and approaches have been validated through short- and mid-term follow-up. Extensive preoperative planning with imaging, accurate intraoperative evaluation of the bone loss, and comprehensive understanding of all the implant options available for the bone loss are paramount to success.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


