Pedro Gabriel Melo de Barros E Silva, Thiago Andrade Macedo, Renato D Lopes, Mariana Y Okada, Tiago Frigini, Patricia O Roveri, Rodrigo Balada, Lucas Silva de Macedo, Valter Furlan
{"title":"支持远程医疗的胸痛网络:8年后对再灌注治疗和临床结果的影响。","authors":"Pedro Gabriel Melo de Barros E Silva, Thiago Andrade Macedo, Renato D Lopes, Mariana Y Okada, Tiago Frigini, Patricia O Roveri, Rodrigo Balada, Lucas Silva de Macedo, Valter Furlan","doi":"10.1089/tmr.2021.0033","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Different approaches of evaluation by cardiologists using telemedicine have the potential of improving care of patients with ST elevation myocardial infarction (STEMI). <b>Objective:</b> To compare the use of pharmacoinvasive strategy and associated clinical outcomes (heart failure [HF] and mortality) among patients with STEMI before and after a program of telemedicine and also according to the level of support by telemedicine. <b>Methods:</b> A chest pain network with the support of a cardiologist through telemedicine was implemented in 2012 in 22 emergency departments without a local cardiac catheterization laboratory. Initially (phase 1 of telemedicine), the decision to discuss the case with the cardiologist was based on the judgment of the emergency physician. At the end of 2018, the use of telemedicine was modified and a dedicated cardiologist was available continuously to discuss systematically all suspected cases (phase 2 of telemedicine). The use of fibrinolytics and the rates of HF and in-hospital mortality were compared among three different periods: pretelemedicine (2011), and phase 1 and phase 2 of the telemedicine program. <b>Results:</b> We evaluated 1034 STEMI patients and after comparing the three phases, we did not find significant differences regarding age, gender, and comorbidities. The use of fibrinolytics before transferring STEMI patients to a percutaneous coronary intervention center (pharmacoinvasive strategy) increased after telemedicine implementation (38% vs. 65.2%; <i>p</i> < 0.01), which was associated with a lower rate of HF (23.9% vs. 14.4%; <i>p</i> = 0.01) and death (7.9% vs. 4.0%; <i>p</i> = 0.05). The in-hospital mortality was lower in phase 2 with systematic evaluation by telemedicine compared with pretelemedicine (7.9% vs. 3.3%; <i>p</i> = 0.04). <b>Conclusion:</b> The implementation of a systematic and organized chest pain protocol, including telemedicine support, was associated with a significant increase in the use of pharmacoinvasive strategy and better clinical patient outcomes in patients with STEMI. Our findings provide important insights on how to improve the management of this high-risk population, reducing the gap between evidence and clinical practice.</p>","PeriodicalId":22295,"journal":{"name":"Telemedicine reports","volume":" ","pages":"284-292"},"PeriodicalIF":0.0000,"publicationDate":"2021-12-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8812289/pdf/","citationCount":"1","resultStr":"{\"title\":\"Chest Pain Network with Support of Telemedicine: Impact on Reperfusion Therapy and Clinical Outcomes After 8 Years of Experience.\",\"authors\":\"Pedro Gabriel Melo de Barros E Silva, Thiago Andrade Macedo, Renato D Lopes, Mariana Y Okada, Tiago Frigini, Patricia O Roveri, Rodrigo Balada, Lucas Silva de Macedo, Valter Furlan\",\"doi\":\"10.1089/tmr.2021.0033\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> Different approaches of evaluation by cardiologists using telemedicine have the potential of improving care of patients with ST elevation myocardial infarction (STEMI). <b>Objective:</b> To compare the use of pharmacoinvasive strategy and associated clinical outcomes (heart failure [HF] and mortality) among patients with STEMI before and after a program of telemedicine and also according to the level of support by telemedicine. <b>Methods:</b> A chest pain network with the support of a cardiologist through telemedicine was implemented in 2012 in 22 emergency departments without a local cardiac catheterization laboratory. Initially (phase 1 of telemedicine), the decision to discuss the case with the cardiologist was based on the judgment of the emergency physician. At the end of 2018, the use of telemedicine was modified and a dedicated cardiologist was available continuously to discuss systematically all suspected cases (phase 2 of telemedicine). The use of fibrinolytics and the rates of HF and in-hospital mortality were compared among three different periods: pretelemedicine (2011), and phase 1 and phase 2 of the telemedicine program. <b>Results:</b> We evaluated 1034 STEMI patients and after comparing the three phases, we did not find significant differences regarding age, gender, and comorbidities. The use of fibrinolytics before transferring STEMI patients to a percutaneous coronary intervention center (pharmacoinvasive strategy) increased after telemedicine implementation (38% vs. 65.2%; <i>p</i> < 0.01), which was associated with a lower rate of HF (23.9% vs. 14.4%; <i>p</i> = 0.01) and death (7.9% vs. 4.0%; <i>p</i> = 0.05). The in-hospital mortality was lower in phase 2 with systematic evaluation by telemedicine compared with pretelemedicine (7.9% vs. 3.3%; <i>p</i> = 0.04). <b>Conclusion:</b> The implementation of a systematic and organized chest pain protocol, including telemedicine support, was associated with a significant increase in the use of pharmacoinvasive strategy and better clinical patient outcomes in patients with STEMI. Our findings provide important insights on how to improve the management of this high-risk population, reducing the gap between evidence and clinical practice.</p>\",\"PeriodicalId\":22295,\"journal\":{\"name\":\"Telemedicine reports\",\"volume\":\" \",\"pages\":\"284-292\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-12-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8812289/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Telemedicine reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1089/tmr.2021.0033\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Telemedicine reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/tmr.2021.0033","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
摘要
背景:心脏病专家使用远程医疗的不同评估方法有可能改善ST段抬高型心肌梗死(STEMI)患者的护理。目的:比较STEMI患者在远程医疗计划前后以及远程医疗支持水平的药物侵入策略和相关临床结果(心力衰竭和死亡率)的使用情况。方法:2012年在22个没有当地心导管实验室的急诊科实施胸痛网络,由心内科医生通过远程医疗提供支持。最初(远程医疗的第一阶段),与心脏病专家讨论病例的决定是基于急诊医生的判断。2018年底,远程医疗的使用进行了修改,并有专门的心脏病专家持续系统地讨论所有疑似病例(远程医疗的第二阶段)。在三个不同时期:远程医疗前(2011年)和远程医疗计划的第一阶段和第二阶段,比较了纤溶剂的使用、心衰率和住院死亡率。结果:我们评估了1034例STEMI患者,在比较了三个阶段后,我们没有发现年龄、性别和合并症方面的显著差异。远程医疗实施后,STEMI患者转至经皮冠状动脉介入治疗中心(药物侵入策略)前使用纤溶剂的比例增加(38% vs. 65.2%;P P = 0.01)和死亡(7.9% vs. 4.0%;p = 0.05)。与远程医疗前相比,通过远程医疗系统评估的第二阶段住院死亡率较低(7.9% vs. 3.3%;p = 0.04)。结论:系统和有组织的胸痛治疗方案的实施,包括远程医疗支持,与STEMI患者药物侵入策略的使用显著增加和更好的临床患者预后相关。我们的发现为如何改善这一高危人群的管理提供了重要的见解,减少了证据与临床实践之间的差距。
Chest Pain Network with Support of Telemedicine: Impact on Reperfusion Therapy and Clinical Outcomes After 8 Years of Experience.
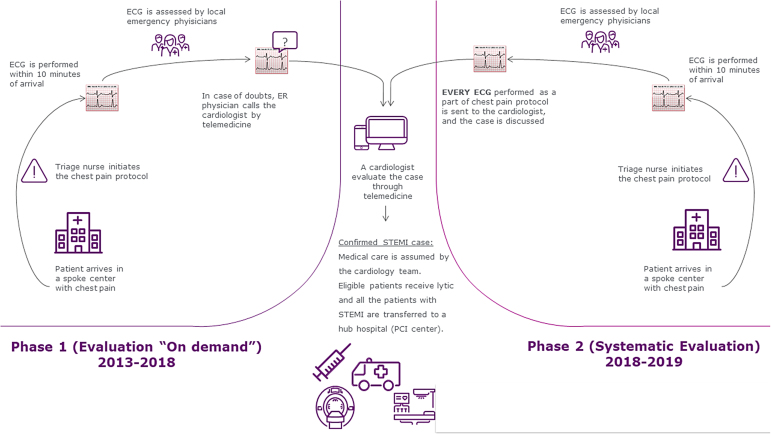
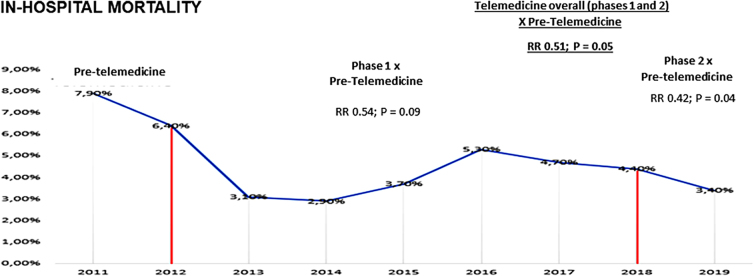
Background: Different approaches of evaluation by cardiologists using telemedicine have the potential of improving care of patients with ST elevation myocardial infarction (STEMI). Objective: To compare the use of pharmacoinvasive strategy and associated clinical outcomes (heart failure [HF] and mortality) among patients with STEMI before and after a program of telemedicine and also according to the level of support by telemedicine. Methods: A chest pain network with the support of a cardiologist through telemedicine was implemented in 2012 in 22 emergency departments without a local cardiac catheterization laboratory. Initially (phase 1 of telemedicine), the decision to discuss the case with the cardiologist was based on the judgment of the emergency physician. At the end of 2018, the use of telemedicine was modified and a dedicated cardiologist was available continuously to discuss systematically all suspected cases (phase 2 of telemedicine). The use of fibrinolytics and the rates of HF and in-hospital mortality were compared among three different periods: pretelemedicine (2011), and phase 1 and phase 2 of the telemedicine program. Results: We evaluated 1034 STEMI patients and after comparing the three phases, we did not find significant differences regarding age, gender, and comorbidities. The use of fibrinolytics before transferring STEMI patients to a percutaneous coronary intervention center (pharmacoinvasive strategy) increased after telemedicine implementation (38% vs. 65.2%; p < 0.01), which was associated with a lower rate of HF (23.9% vs. 14.4%; p = 0.01) and death (7.9% vs. 4.0%; p = 0.05). The in-hospital mortality was lower in phase 2 with systematic evaluation by telemedicine compared with pretelemedicine (7.9% vs. 3.3%; p = 0.04). Conclusion: The implementation of a systematic and organized chest pain protocol, including telemedicine support, was associated with a significant increase in the use of pharmacoinvasive strategy and better clinical patient outcomes in patients with STEMI. Our findings provide important insights on how to improve the management of this high-risk population, reducing the gap between evidence and clinical practice.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


