{"title":"基于fibroscan的评分系统用于缩小非酒精性脂肪性肝病合并症的风险组","authors":"Kouichi Miura, Hiroshi Maeda, Naoki Morimoto, Shunji Watanabe, Mamiko Tsukui, Yoshinari Takaoka, Hiroaki Nomoto, Rie Goka, Kazuhiko Kotani, Hironori Yamamoto","doi":"10.4291/wjgp.v13.i3.96","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Vibration-controlled transient elastography (VCTE) is proposed as a second step of examination to assess liver fibrosis in patients with nonalcoholic fatty liver disease (NAFLD) after triaging by the fibrosis-4 (FIB-4) index. Recently, VCTE-based scoring systems, including FibroScan-AST (FAST), Agile 3+, and Agile 4, emerged to determine the status of NAFLD. However, the significance of these scoring systems remains unknown in narrowing the high-risk group of NAFLD patients with comorbidities, including hepatocellular carcinoma (HCC) and esophagogastric varices (EGV).</p><p><strong>Aim: </strong>To clarify the significance of VCTE-based scoring systems to narrow the high-risk group of NAFLD patients with comorbidities.</p><p><strong>Methods: </strong>We performed a cross-sectional study to investigate the usefulness of VCTE-based scoring systems and other fibrosis markers to narrow the high-risk group of patients with NAFLD. FIB-4 index was used for the first triage. Risk groups of FAST, Agile 3+, and Agile 4 were stratified according to the published data. Among the 191 patients with NAFLD, there were 26 (14%) and 25 patients (13%) with HCC and EGV, respectively.</p><p><strong>Results: </strong>When 1.3 was used as a cutoff value, the FIB-4 index narrowed the risk group to 120 patients, in which all patients with HCC and/or EGV were included. High risk group of Agile 3+ could subsequently narrow the risk group. The prevalence of HCC and EGV at this step were 33% (26/80) and 31% (25/80), respectively. In further narrowing of EGV, Agile 4 aggregated the patients with EGV into 43 patients, of whom 23 (53%) had EGV. FAST failed to narrow the risk group of patients with comorbidities. When 2.6 was used as a cutoff value of the FIB-4 index, three patients with HCC and two patients with EGV were missed at the first triage.</p><p><strong>Conclusion: </strong>Agile 3+ and Agile 4 are useful to narrow the NAFLD patient group, in which patients may have HCC and/or EGV.</p>","PeriodicalId":23760,"journal":{"name":"World Journal of Gastrointestinal Pathophysiology","volume":"13 3","pages":"96-106"},"PeriodicalIF":0.0000,"publicationDate":"2022-05-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/af/b3/WJGP-13-96.PMC9157683.pdf","citationCount":"5","resultStr":"{\"title\":\"Utility of FibroScan-based scoring systems to narrow the risk group of nonalcoholic fatty liver disease with comorbidities.\",\"authors\":\"Kouichi Miura, Hiroshi Maeda, Naoki Morimoto, Shunji Watanabe, Mamiko Tsukui, Yoshinari Takaoka, Hiroaki Nomoto, Rie Goka, Kazuhiko Kotani, Hironori Yamamoto\",\"doi\":\"10.4291/wjgp.v13.i3.96\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Vibration-controlled transient elastography (VCTE) is proposed as a second step of examination to assess liver fibrosis in patients with nonalcoholic fatty liver disease (NAFLD) after triaging by the fibrosis-4 (FIB-4) index. Recently, VCTE-based scoring systems, including FibroScan-AST (FAST), Agile 3+, and Agile 4, emerged to determine the status of NAFLD. However, the significance of these scoring systems remains unknown in narrowing the high-risk group of NAFLD patients with comorbidities, including hepatocellular carcinoma (HCC) and esophagogastric varices (EGV).</p><p><strong>Aim: </strong>To clarify the significance of VCTE-based scoring systems to narrow the high-risk group of NAFLD patients with comorbidities.</p><p><strong>Methods: </strong>We performed a cross-sectional study to investigate the usefulness of VCTE-based scoring systems and other fibrosis markers to narrow the high-risk group of patients with NAFLD. FIB-4 index was used for the first triage. Risk groups of FAST, Agile 3+, and Agile 4 were stratified according to the published data. Among the 191 patients with NAFLD, there were 26 (14%) and 25 patients (13%) with HCC and EGV, respectively.</p><p><strong>Results: </strong>When 1.3 was used as a cutoff value, the FIB-4 index narrowed the risk group to 120 patients, in which all patients with HCC and/or EGV were included. High risk group of Agile 3+ could subsequently narrow the risk group. The prevalence of HCC and EGV at this step were 33% (26/80) and 31% (25/80), respectively. In further narrowing of EGV, Agile 4 aggregated the patients with EGV into 43 patients, of whom 23 (53%) had EGV. FAST failed to narrow the risk group of patients with comorbidities. When 2.6 was used as a cutoff value of the FIB-4 index, three patients with HCC and two patients with EGV were missed at the first triage.</p><p><strong>Conclusion: </strong>Agile 3+ and Agile 4 are useful to narrow the NAFLD patient group, in which patients may have HCC and/or EGV.</p>\",\"PeriodicalId\":23760,\"journal\":{\"name\":\"World Journal of Gastrointestinal Pathophysiology\",\"volume\":\"13 3\",\"pages\":\"96-106\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-05-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/af/b3/WJGP-13-96.PMC9157683.pdf\",\"citationCount\":\"5\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Gastrointestinal Pathophysiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4291/wjgp.v13.i3.96\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastrointestinal Pathophysiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4291/wjgp.v13.i3.96","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Utility of FibroScan-based scoring systems to narrow the risk group of nonalcoholic fatty liver disease with comorbidities.
Background: Vibration-controlled transient elastography (VCTE) is proposed as a second step of examination to assess liver fibrosis in patients with nonalcoholic fatty liver disease (NAFLD) after triaging by the fibrosis-4 (FIB-4) index. Recently, VCTE-based scoring systems, including FibroScan-AST (FAST), Agile 3+, and Agile 4, emerged to determine the status of NAFLD. However, the significance of these scoring systems remains unknown in narrowing the high-risk group of NAFLD patients with comorbidities, including hepatocellular carcinoma (HCC) and esophagogastric varices (EGV).
Aim: To clarify the significance of VCTE-based scoring systems to narrow the high-risk group of NAFLD patients with comorbidities.
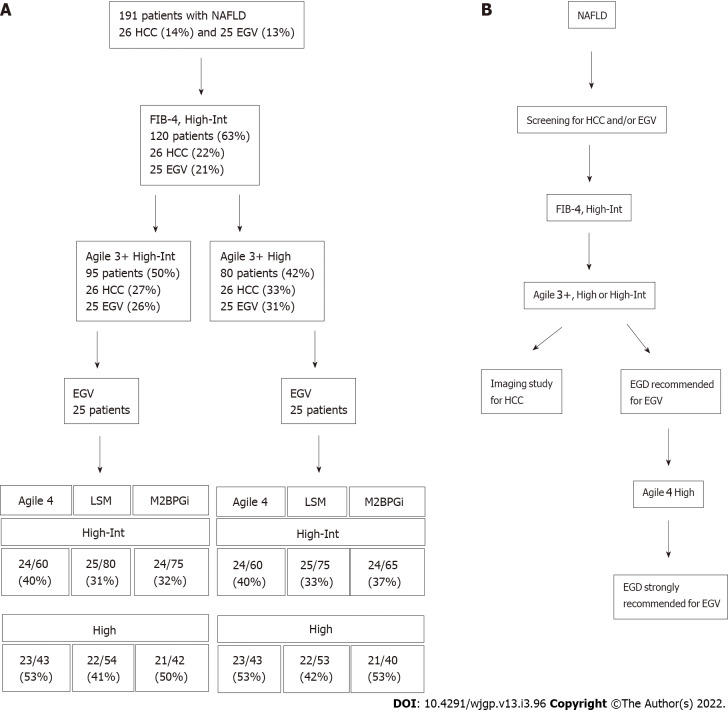
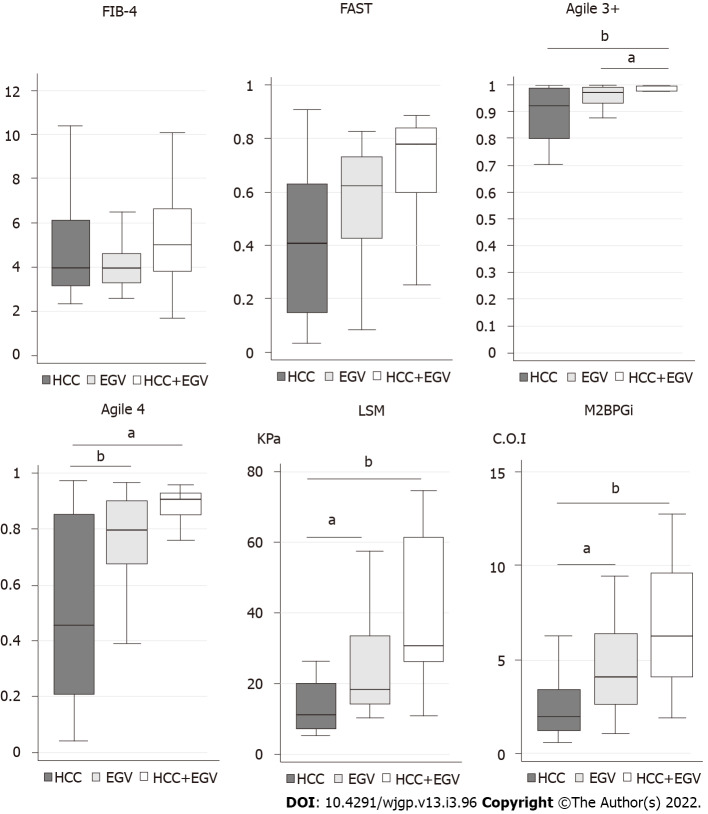
Methods: We performed a cross-sectional study to investigate the usefulness of VCTE-based scoring systems and other fibrosis markers to narrow the high-risk group of patients with NAFLD. FIB-4 index was used for the first triage. Risk groups of FAST, Agile 3+, and Agile 4 were stratified according to the published data. Among the 191 patients with NAFLD, there were 26 (14%) and 25 patients (13%) with HCC and EGV, respectively.
Results: When 1.3 was used as a cutoff value, the FIB-4 index narrowed the risk group to 120 patients, in which all patients with HCC and/or EGV were included. High risk group of Agile 3+ could subsequently narrow the risk group. The prevalence of HCC and EGV at this step were 33% (26/80) and 31% (25/80), respectively. In further narrowing of EGV, Agile 4 aggregated the patients with EGV into 43 patients, of whom 23 (53%) had EGV. FAST failed to narrow the risk group of patients with comorbidities. When 2.6 was used as a cutoff value of the FIB-4 index, three patients with HCC and two patients with EGV were missed at the first triage.
Conclusion: Agile 3+ and Agile 4 are useful to narrow the NAFLD patient group, in which patients may have HCC and/or EGV.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


