Anais Alonso, Shoma Barat, Helen Kennedy, Meredith Potter, Nayef Alzahrani, David Morris
{"title":"输尿管再植术患者行细胞减少术的危险因素和临床结果。","authors":"Anais Alonso, Shoma Barat, Helen Kennedy, Meredith Potter, Nayef Alzahrani, David Morris","doi":"10.1515/pp-2021-0130","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>There are currently scarce data exploring ureteric reimplantation (UR) during cytoreductive surgery (CRS).</p><p><strong>Methods: </strong>We identified patients undergoing CRS for peritoneal surface malignancies (PSM) of any origin at a single high-volume unit. UR was defined as ureteroureterostomy, transureterouretostomy, ureteroneocystostomy, ureterosigmoidostomy or ileal conduit performed during CRS. Peri-operative outcomes, long-term survival and risk factors for requiring UR were analysed.</p><p><strong>Results: </strong>Seven hundred and sixty-seven CRSs were identified. Twenty-three (3.0%) procedures involved UR. Bladder resection and colorectal cancer (CRC) were associated with increased risk of UR (bladder resection: OR 12.90, 95% CI 4.91-33.90, p<0.001; CRC: OR 2.51, 95% CI 1.05-6.01, p=0.038). UR did not increase the risk of Grade III-IV morbidity or mortality. The rate of ureteric leak was 3/23 (13.0%) in the UR group. Mean survival was equivocal in patients with CRC (58.14 vs. 34.25 months, p=0.441) but significantly lower in those with high-grade appendiceal mucinous neoplasm (HAMN) undergoing UR (73.98 vs. 30.90 months, p=0.029).</p><p><strong>Conclusions: </strong>UR during CRS does not increase major morbidity or mortality for carefully selected patients, and is associated with low rates of urologic complications. Whilst decreased survival was apparent in patients with HAMN undergoing UR, it is unclear whether this relationship is causal.</p>","PeriodicalId":20231,"journal":{"name":"Pleura and Peritoneum","volume":"6 4","pages":"155-160"},"PeriodicalIF":2.4000,"publicationDate":"2021-11-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8719446/pdf/","citationCount":"0","resultStr":"{\"title\":\"Risk factors and clinical outcomes in patients undergoing cytoreductive surgery with concomitant ureteric reimplantation.\",\"authors\":\"Anais Alonso, Shoma Barat, Helen Kennedy, Meredith Potter, Nayef Alzahrani, David Morris\",\"doi\":\"10.1515/pp-2021-0130\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>There are currently scarce data exploring ureteric reimplantation (UR) during cytoreductive surgery (CRS).</p><p><strong>Methods: </strong>We identified patients undergoing CRS for peritoneal surface malignancies (PSM) of any origin at a single high-volume unit. UR was defined as ureteroureterostomy, transureterouretostomy, ureteroneocystostomy, ureterosigmoidostomy or ileal conduit performed during CRS. Peri-operative outcomes, long-term survival and risk factors for requiring UR were analysed.</p><p><strong>Results: </strong>Seven hundred and sixty-seven CRSs were identified. Twenty-three (3.0%) procedures involved UR. Bladder resection and colorectal cancer (CRC) were associated with increased risk of UR (bladder resection: OR 12.90, 95% CI 4.91-33.90, p<0.001; CRC: OR 2.51, 95% CI 1.05-6.01, p=0.038). UR did not increase the risk of Grade III-IV morbidity or mortality. The rate of ureteric leak was 3/23 (13.0%) in the UR group. Mean survival was equivocal in patients with CRC (58.14 vs. 34.25 months, p=0.441) but significantly lower in those with high-grade appendiceal mucinous neoplasm (HAMN) undergoing UR (73.98 vs. 30.90 months, p=0.029).</p><p><strong>Conclusions: </strong>UR during CRS does not increase major morbidity or mortality for carefully selected patients, and is associated with low rates of urologic complications. Whilst decreased survival was apparent in patients with HAMN undergoing UR, it is unclear whether this relationship is causal.</p>\",\"PeriodicalId\":20231,\"journal\":{\"name\":\"Pleura and Peritoneum\",\"volume\":\"6 4\",\"pages\":\"155-160\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2021-11-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8719446/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pleura and Peritoneum\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1515/pp-2021-0130\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/12/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pleura and Peritoneum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1515/pp-2021-0130","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/12/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
目的:目前关于细胞减少手术(CRS)中输尿管再植(UR)的研究资料很少。方法:我们在单个高容量单位中确定了任何来源的腹膜表面恶性肿瘤(PSM)接受CRS的患者。UR定义为CRS中进行的输尿管输尿管造口术、经输尿管输尿管造口术、输尿管膀胱造口术、输尿管乙状结肠造口术或回肠导管造口术。分析围手术期结局、长期生存和需要UR的危险因素。结果:共鉴定出767个crs。23例(3.0%)手术涉及UR。膀胱切除术和结直肠癌(CRC)与尿路风险增加相关(膀胱切除术:OR 12.90, 95% CI 4.91-33.90, p)结论:对于精心挑选的患者,CRS期间尿路不会增加主要发病率或死亡率,并且与泌尿系统并发症发生率低相关。虽然HAMN患者接受尿路治疗的生存率明显下降,但尚不清楚这种关系是否有因果关系。
Risk factors and clinical outcomes in patients undergoing cytoreductive surgery with concomitant ureteric reimplantation.
Objectives: There are currently scarce data exploring ureteric reimplantation (UR) during cytoreductive surgery (CRS).
Methods: We identified patients undergoing CRS for peritoneal surface malignancies (PSM) of any origin at a single high-volume unit. UR was defined as ureteroureterostomy, transureterouretostomy, ureteroneocystostomy, ureterosigmoidostomy or ileal conduit performed during CRS. Peri-operative outcomes, long-term survival and risk factors for requiring UR were analysed.
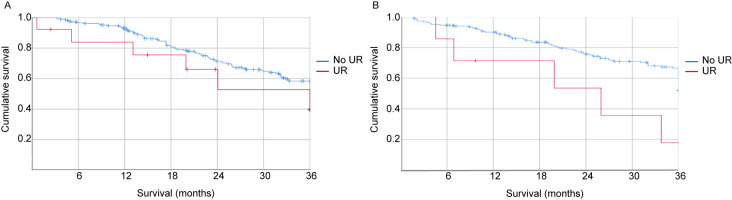
Results: Seven hundred and sixty-seven CRSs were identified. Twenty-three (3.0%) procedures involved UR. Bladder resection and colorectal cancer (CRC) were associated with increased risk of UR (bladder resection: OR 12.90, 95% CI 4.91-33.90, p<0.001; CRC: OR 2.51, 95% CI 1.05-6.01, p=0.038). UR did not increase the risk of Grade III-IV morbidity or mortality. The rate of ureteric leak was 3/23 (13.0%) in the UR group. Mean survival was equivocal in patients with CRC (58.14 vs. 34.25 months, p=0.441) but significantly lower in those with high-grade appendiceal mucinous neoplasm (HAMN) undergoing UR (73.98 vs. 30.90 months, p=0.029).
Conclusions: UR during CRS does not increase major morbidity or mortality for carefully selected patients, and is associated with low rates of urologic complications. Whilst decreased survival was apparent in patients with HAMN undergoing UR, it is unclear whether this relationship is causal.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


