金钱激励和同伴转诊促进中国男男性行为者艾滋病病毒自检二次分发:一项随机对照试验
摘要
背景:基于数字网络的方法可能会加强艾滋病毒自我检测(HIVST)试剂盒的同伴分发,但需要能够优化这种方法的干预措施。我们的目的是评估金钱激励和同伴推荐是否可以改善中国男男性行为者(MSM)中hiv的二次分发方案。方法和研究结果:在2019年10月21日至2020年9月14日期间,在309名(定义为指数参与者)中进行了一项3组随机对照单盲试验,这些人在出生时被指定为男性,年龄在18岁或以上,曾经发生过男性间的性行为,愿意在线订购艾滋病毒检测试剂盒,并同意在线接受调查。我们将指标参与者随机分配到三个组中的一个:(1)标准二次分布(对照组)组(n = 102);(2)有货币激励的二次分配(SD-M)组(n = 103);(3)有货币激励加同伴推荐的二次分配(SD-M-PR)组(n = 104)。鼓励三个组的指数参与者在线订购艾滋病毒传播工具包,并在其社交网络中分发给成员。直接从索引参与者或通过索引男男性行为者的同行推荐链接获得工具包的成员被定义为更改者。两个干预组的指数参与者可以在线获得固定奖励(3美元),用于通过每个唯一更改将验证的测试结果上传到数字平台。SD-M-PR组的索引参与者还可以有一个个性化的同伴推荐链接,以便更改在线订购工具包。指数参与者和更改者都需要支付可退还的押金(15美元)来订购工具包。所有指数参与者在订购工具包后都被分配了一个为期3个月的在线跟踪调查。主要结果是每组中指标参与者的平均改变数和每组中指标参与者的平均新测试改变数。这些评估使用零膨胀负二项回归,以确定在平均数量的改变和平均数量的新测试的改变由指数参与者的动机组的差异。在意向治疗基础上进行分析。我们还从医疗服务提供者的角度进行了为期3个月的微观成本经济评估。由指标被试引起的独特改变数,对照组平均为0.57±0.96(均数±标准差[SD]), SD- m组为0.98±1.38(均数差[MD] = 0.41), SD- m - pr组为1.78±2.05 (MD = 1.21)。对照组新测改变数为0.16±0.39 (mean±SD), SD- m组为0.41±0.73 (MD = 0.25), SD- m - pr组为0.57±0.91 (MD = 0.41)。结果表明,干预组的指数参与者更有可能激发独特的测试改变(对照与SD-M:发病率比[IRR = 2.98, 95% CI = 1.82 ~ 4.89, p值< 0.001;对照SD-M- pr: IRR = 3.26, 95% CI = 2.29 ~ 4.63, p值< 0.001)和新检测的改变者(对照SD-M: IRR = 4.22, 95% CI = 1.93 ~ 9.23, p值< 0.001;对照SD-M-PR: IRR = 3.49, 95% CI = 1.92 ~ 6.37, p值< 0.001)进行hiv - st。对照组新测者比例为28%,SD-M组为42%,SD-M- pr组为32%。共有18名测试者(3名指数参与者和15名改变者)被检测为HIV阳性,三组之间改变者的HIV反应率相似。794名测试人员的总成本为19,485.97美元,其中包括450名指数参与者和344名更改测试人员。总的来说,每个测试人员的平均成本是24.54美元,每个变更测试人员的平均成本是56.65美元。尽管SD-M- pr的效果更大,但在测试的改变和新测试的改变方面,平均而言,单独的金钱激励(SD-M组)比同伴推荐的金钱激励(SD-M- pr组)更具成本效益。与对照组相比,SD-M组每增加一个alter tester的成本为14.90美元,SD-M- pr组为16.61美元。对于新测试的改变,SD-M组每增加一个改变的成本为24.65美元,SD-M- pr组为49.07美元。研究期间未报告与研究相关的不良事件。限制包括数字网络方法可能会忽视缺乏互联网接入的个人。结论:单纯的金钱激励和金钱激励与同伴转诊相结合的干预可以促进hiv在男男性行为者中的二次分布。金钱奖励也可以通过鼓励男男性行为者通过二次分发进行首次检测来扩大艾滋病毒检测。这种基于社交网络的数字方法可以扩展到其他公共卫生研究,特别是在2019年冠状病毒病(COVID-19)时代。试验注册:中国临床试验注册中心(ChiCTR) ChiCTR1900025433。
Background: Digital network-based methods may enhance peer distribution of HIV self-testing (HIVST) kits, but interventions that can optimize this approach are needed. We aimed to assess whether monetary incentives and peer referral could improve a secondary distribution program for HIVST among men who have sex with men (MSM) in China.
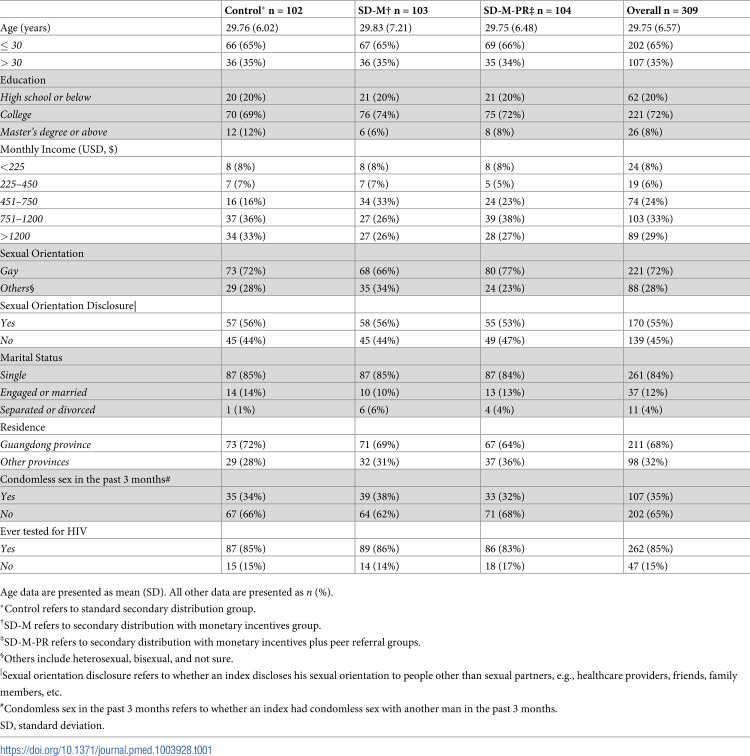
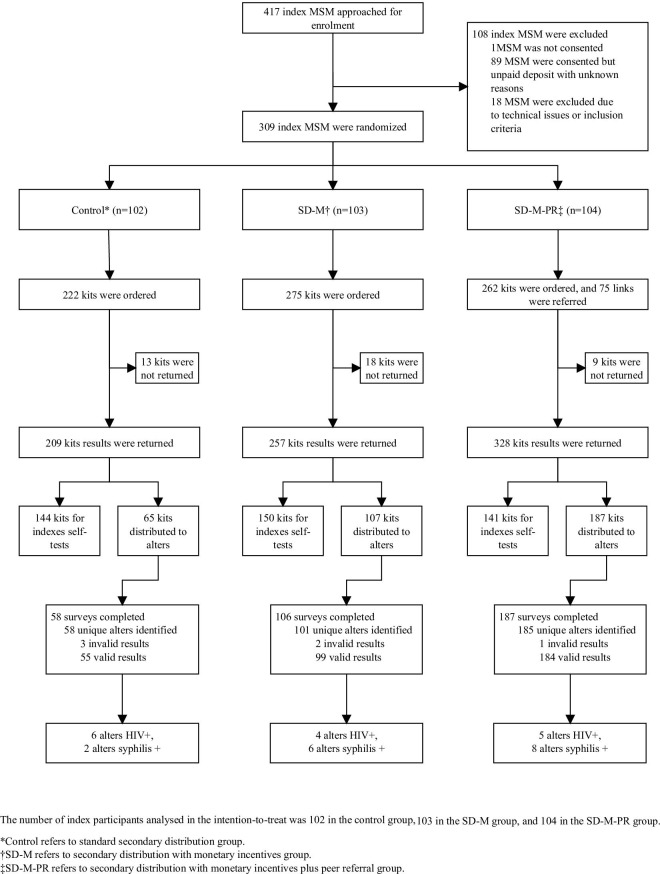
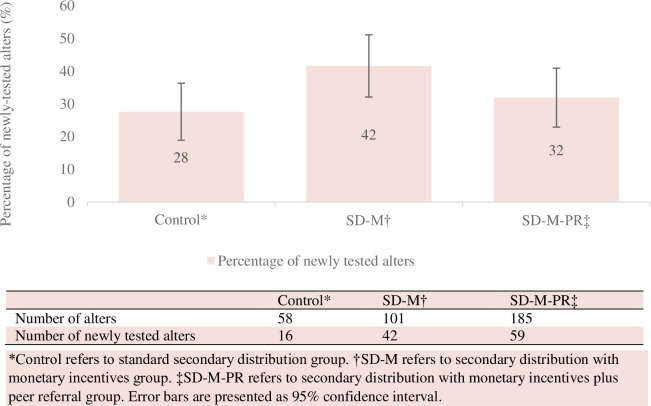
Methods and findings: Between October 21, 2019 and September 14, 2020, a 3-arm randomized controlled, single-blinded trial was conducted online among 309 individuals (defined as index participants) who were assigned male at birth, aged 18 years or older, ever had male-to-male sex, willing to order HIVST kits online, and consented to take surveys online. We randomly assigned index participants into one of the 3 arms: (1) standard secondary distribution (control) group (n = 102); (2) secondary distribution with monetary incentives (SD-M) group (n = 103); and (3) secondary distribution with monetary incentives plus peer referral (SD-M-PR) group (n = 104). Index participants in 3 groups were encouraged to order HIVST kits online and distribute to members within their social networks. Members who received kits directly from index participants or through peer referral links from index MSM were defined as alters. Index participants in the 2 intervention groups could receive a fixed incentive ($3 USD) online for the verified test result uploaded to the digital platform by each unique alter. Index participants in the SD-M-PR group could additionally have a personalized peer referral link for alters to order kits online. Both index participants and alters needed to pay a refundable deposit ($15 USD) for ordering a kit. All index participants were assigned an online 3-month follow-up survey after ordering kits. The primary outcomes were the mean number of alters motivated by index participants in each arm and the mean number of newly tested alters motivated by index participants in each arm. These were assessed using zero-inflated negative binomial regression to determine the group differences in the mean number of alters and the mean number of newly tested alters motivated by index participants. Analyses were performed on an intention-to-treat basis. We also conducted an economic evaluation using microcosting from a health provider perspective with a 3-month time horizon. The mean number of unique tested alters motivated by index participants was 0.57 ± 0.96 (mean ± standard deviation [SD]) in the control group, compared with 0.98 ± 1.38 in the SD-M group (mean difference [MD] = 0.41),and 1.78 ± 2.05 in the SD-M-PR group (MD = 1.21). The mean number of newly tested alters motivated by index participants was 0.16 ± 0.39 (mean ± SD) in the control group, compared with 0.41 ± 0.73 in the SD-M group (MD = 0.25) and 0.57 ± 0.91 in the SD-M-PR group (MD = 0.41), respectively. Results indicated that index participants in intervention arms were more likely to motivate unique tested alters (control versus SD-M: incidence rate ratio [IRR = 2.98, 95% CI = 1.82 to 4.89, p-value < 0.001; control versus SD-M-PR: IRR = 3.26, 95% CI = 2.29 to 4.63, p-value < 0.001) and newly tested alters (control versus SD-M: IRR = 4.22, 95% CI = 1.93 to 9.23, p-value < 0.001; control versus SD-M-PR: IRR = 3.49, 95% CI = 1.92 to 6.37, p-value < 0.001) to conduct HIVST. The proportion of newly tested testers among alters was 28% in the control group, 42% in the SD-M group, and 32% in the SD-M-PR group. A total of 18 testers (3 index participants and 15 alters) tested as HIV positive, and the HIV reactive rates for alters were similar between the 3 groups. The total costs were $19,485.97 for 794 testers, including 450 index participants and 344 alter testers. Overall, the average cost per tester was $24.54, and the average cost per alter tester was $56.65. Monetary incentives alone (SD-M group) were more cost-effective than monetary incentives with peer referral (SD-M-PR group) on average in terms of alters tested and newly tested alters, despite SD-M-PR having larger effects. Compared to the control group, the cost for one more alter tester in the SD-M group was $14.90 and $16.61 in the SD-M-PR group. For newly tested alters, the cost of one more alter in the SD-M group was $24.65 and $49.07 in the SD-M-PR group. No study-related adverse events were reported during the study. Limitations include the digital network approach might neglect individuals who lack internet access.
Conclusions: Monetary incentives alone and the combined intervention of monetary incentives and peer referral can promote the secondary distribution of HIVST among MSM. Monetary incentives can also expand HIV testing by encouraging first-time testing through secondary distribution by MSM. This social network-based digital approach can be expanded to other public health research, especially in the era of the Coronavirus Disease 2019 (COVID-19).
Trial registration: Chinese Clinical Trial Registry (ChiCTR) ChiCTR1900025433.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:



