{"title":"急性淋巴细胞白血病的广泛髓-颈胸病变。","authors":"Mitsuko Nakajima, Mathilde Pauls, Sanjeev Rajakulendran","doi":"10.3988/jcn.2022.18.1.105","DOIUrl":null,"url":null,"abstract":"Dear Editor, The etiology of longitudinal spinal cord lesions includes inflammation, vascular causes, and malignancy. Acute leukemia in the spinal cord has been reported previously, but it usually only presents with constitutional symptoms and peripheral evidence of the disease. We report a case of leukemia presenting initially as spinal cord disease with imaging revealing a longitudinally extensive medullo-cervicothoracic lesion. A 73-year-old female presented with subacute progressive weakness in her arms and legs, numbness in her hands, and sphincteric disturbance over several weeks, which occurred during a lockdown period due to the coronavirus crisis in early 2020. She reported no bulbar symptoms or pain. She was systemically well with no history of fevers, weight loss, night sweats, recurrent infections, or bruising. Her breathing was unaffected. Her past medical history consisted of type 2 diabetes mellitus, hypothyroidism, squamous cell carcinoma, and lumbar spinal fusion. Salient findings in a neurological examination were asymmetric quadriparesis (left>right), spasticity, and hyperreflexia. There were no abnormal cranial nerve signs. A systemic examination produced unremarkable findings. Magnetic resonance imaging (MRI) of the neuraxis revealed a longitudinally extensive lesion that began at the level of the lower medulla and terminated at T3 (Fig. 1). The lesion exhibited heterogeneous enhancement after administering a contrast agent. The spinal cord appeared swollen, particularly in the cervical region. The differential diagnosis included an inflammatory etiology, malignancy, and a high-level (intracranial/cervicomedullary) arteriovenous fistula, which was less likely but still thought worthy of consideration. The findings of head MRI with contrast agent were normal. Screening blood tests demonstrated only a slightly elevated white blood cell count (13.4× 109/L), with no anemia and normal inflammatory markers. Screening revealed negativity for autoantibodies (including anti-aquaporin-4 and anti-myelin oligodendrocyte glycoprotein antibodies). A cerebrospinal fluid (CSF) examination identified a white blood cell count of 3/mL, elevated protein at 0.94 g/L, normal glucose, and matched oligoclonal bands with isoelectric focussing. The CSF and serum IgG index was 1.53. The presence of lymphoblasts in the CSF was suggestive of acute leukemia, most probably of B-lymphoid lineage, supported by demonstration of CD45-CD34+CD19+CD10blasts in CSF flow cytometry. Fluorodeoxyglucose positron-emission tomography did not demonstrate abnormal uptake in the bone marrow (BM). BM aspirate showed normal lymphocyte numbers and morphology, and the absence of lymphoblasts. Flow cytometry revealed a small population of phenotypically abnormal B cells, with CD45+CD34+CD38loCD19+CD10+sIg+ (lambda restricted) that accounted for 0.21% BM cellularity. The abnormal cells in CSF were CD45-, indicative of a precursor status. This was distinguished from primary CNS lymphoma by the presence of lymphoblast cells, and by the absence of clonal immunoglobulin heavy-chain and kappa Mitsuko Nakajima Mathilde Pauls Sanjeev Rajakulendran","PeriodicalId":324902,"journal":{"name":"Journal of Clinical Neurology (Seoul, Korea)","volume":" ","pages":"105-107"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/af/f8/jcn-18-105.PMC8762490.pdf","citationCount":"0","resultStr":"{\"title\":\"Extensive Medullo-Cervicothoracic Lesion in Acute Lymphoblastic Leukemia.\",\"authors\":\"Mitsuko Nakajima, Mathilde Pauls, Sanjeev Rajakulendran\",\"doi\":\"10.3988/jcn.2022.18.1.105\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Dear Editor, The etiology of longitudinal spinal cord lesions includes inflammation, vascular causes, and malignancy. Acute leukemia in the spinal cord has been reported previously, but it usually only presents with constitutional symptoms and peripheral evidence of the disease. We report a case of leukemia presenting initially as spinal cord disease with imaging revealing a longitudinally extensive medullo-cervicothoracic lesion. A 73-year-old female presented with subacute progressive weakness in her arms and legs, numbness in her hands, and sphincteric disturbance over several weeks, which occurred during a lockdown period due to the coronavirus crisis in early 2020. She reported no bulbar symptoms or pain. She was systemically well with no history of fevers, weight loss, night sweats, recurrent infections, or bruising. Her breathing was unaffected. Her past medical history consisted of type 2 diabetes mellitus, hypothyroidism, squamous cell carcinoma, and lumbar spinal fusion. Salient findings in a neurological examination were asymmetric quadriparesis (left>right), spasticity, and hyperreflexia. There were no abnormal cranial nerve signs. A systemic examination produced unremarkable findings. Magnetic resonance imaging (MRI) of the neuraxis revealed a longitudinally extensive lesion that began at the level of the lower medulla and terminated at T3 (Fig. 1). The lesion exhibited heterogeneous enhancement after administering a contrast agent. The spinal cord appeared swollen, particularly in the cervical region. The differential diagnosis included an inflammatory etiology, malignancy, and a high-level (intracranial/cervicomedullary) arteriovenous fistula, which was less likely but still thought worthy of consideration. The findings of head MRI with contrast agent were normal. Screening blood tests demonstrated only a slightly elevated white blood cell count (13.4× 109/L), with no anemia and normal inflammatory markers. Screening revealed negativity for autoantibodies (including anti-aquaporin-4 and anti-myelin oligodendrocyte glycoprotein antibodies). A cerebrospinal fluid (CSF) examination identified a white blood cell count of 3/mL, elevated protein at 0.94 g/L, normal glucose, and matched oligoclonal bands with isoelectric focussing. The CSF and serum IgG index was 1.53. The presence of lymphoblasts in the CSF was suggestive of acute leukemia, most probably of B-lymphoid lineage, supported by demonstration of CD45-CD34+CD19+CD10blasts in CSF flow cytometry. Fluorodeoxyglucose positron-emission tomography did not demonstrate abnormal uptake in the bone marrow (BM). BM aspirate showed normal lymphocyte numbers and morphology, and the absence of lymphoblasts. Flow cytometry revealed a small population of phenotypically abnormal B cells, with CD45+CD34+CD38loCD19+CD10+sIg+ (lambda restricted) that accounted for 0.21% BM cellularity. The abnormal cells in CSF were CD45-, indicative of a precursor status. This was distinguished from primary CNS lymphoma by the presence of lymphoblast cells, and by the absence of clonal immunoglobulin heavy-chain and kappa Mitsuko Nakajima Mathilde Pauls Sanjeev Rajakulendran\",\"PeriodicalId\":324902,\"journal\":{\"name\":\"Journal of Clinical Neurology (Seoul, Korea)\",\"volume\":\" \",\"pages\":\"105-107\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/af/f8/jcn-18-105.PMC8762490.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Neurology (Seoul, Korea)\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3988/jcn.2022.18.1.105\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Neurology (Seoul, Korea)","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3988/jcn.2022.18.1.105","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Extensive Medullo-Cervicothoracic Lesion in Acute Lymphoblastic Leukemia.
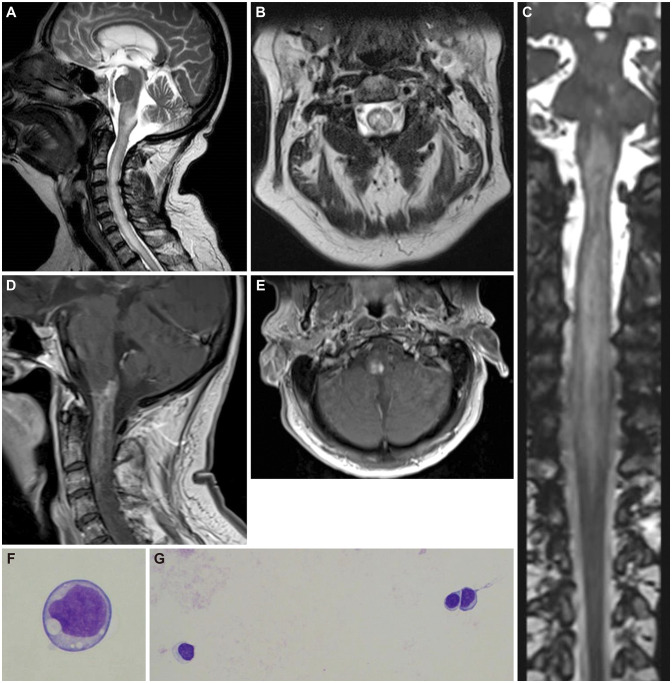
Dear Editor, The etiology of longitudinal spinal cord lesions includes inflammation, vascular causes, and malignancy. Acute leukemia in the spinal cord has been reported previously, but it usually only presents with constitutional symptoms and peripheral evidence of the disease. We report a case of leukemia presenting initially as spinal cord disease with imaging revealing a longitudinally extensive medullo-cervicothoracic lesion. A 73-year-old female presented with subacute progressive weakness in her arms and legs, numbness in her hands, and sphincteric disturbance over several weeks, which occurred during a lockdown period due to the coronavirus crisis in early 2020. She reported no bulbar symptoms or pain. She was systemically well with no history of fevers, weight loss, night sweats, recurrent infections, or bruising. Her breathing was unaffected. Her past medical history consisted of type 2 diabetes mellitus, hypothyroidism, squamous cell carcinoma, and lumbar spinal fusion. Salient findings in a neurological examination were asymmetric quadriparesis (left>right), spasticity, and hyperreflexia. There were no abnormal cranial nerve signs. A systemic examination produced unremarkable findings. Magnetic resonance imaging (MRI) of the neuraxis revealed a longitudinally extensive lesion that began at the level of the lower medulla and terminated at T3 (Fig. 1). The lesion exhibited heterogeneous enhancement after administering a contrast agent. The spinal cord appeared swollen, particularly in the cervical region. The differential diagnosis included an inflammatory etiology, malignancy, and a high-level (intracranial/cervicomedullary) arteriovenous fistula, which was less likely but still thought worthy of consideration. The findings of head MRI with contrast agent were normal. Screening blood tests demonstrated only a slightly elevated white blood cell count (13.4× 109/L), with no anemia and normal inflammatory markers. Screening revealed negativity for autoantibodies (including anti-aquaporin-4 and anti-myelin oligodendrocyte glycoprotein antibodies). A cerebrospinal fluid (CSF) examination identified a white blood cell count of 3/mL, elevated protein at 0.94 g/L, normal glucose, and matched oligoclonal bands with isoelectric focussing. The CSF and serum IgG index was 1.53. The presence of lymphoblasts in the CSF was suggestive of acute leukemia, most probably of B-lymphoid lineage, supported by demonstration of CD45-CD34+CD19+CD10blasts in CSF flow cytometry. Fluorodeoxyglucose positron-emission tomography did not demonstrate abnormal uptake in the bone marrow (BM). BM aspirate showed normal lymphocyte numbers and morphology, and the absence of lymphoblasts. Flow cytometry revealed a small population of phenotypically abnormal B cells, with CD45+CD34+CD38loCD19+CD10+sIg+ (lambda restricted) that accounted for 0.21% BM cellularity. The abnormal cells in CSF were CD45-, indicative of a precursor status. This was distinguished from primary CNS lymphoma by the presence of lymphoblast cells, and by the absence of clonal immunoglobulin heavy-chain and kappa Mitsuko Nakajima Mathilde Pauls Sanjeev Rajakulendran

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


