{"title":"运动头痛与颈外动脉动静脉瘘相关。","authors":"Kyusik Kang, Jae Hoon Kim, Byung-Kun Kim","doi":"10.3988/jcn.2022.18.1.93","DOIUrl":null,"url":null,"abstract":"Dear Editor, Exercise headache is a headache provoked by exercise or exertion.1 Symptomatic causes of exercise headache include subarachnoid hemorrhage, arterial dissection, reversible cerebral vasoconstriction syndrome, and, less commonly, space-occupying lesions, sinusitis, Chiari malformation, and pheochromocytoma.1 We report a patient with recurrent exercise-induced and coital headaches associated with an arteriovenous fistula between the external carotid artery and the external jugular vein. A 27-year old male presented with a 15-year history of severe left occipital headaches induced by physical exercise (e.g., anaerobic leg exercises at a gym) and a 3-year history of headaches during coitus. The exercise-induced headaches peaked within 10 minutes, and then subsided over a couple of hours. He described a left occipital throbbing without associated nausea or light or noise sensitivity. The intensity was 8/10 at about 10 minutes after the onset. The headaches during coitus increased with the degree of sexual excitement. Coughing and other Valsalva (straining) maneuvers did not provoke the headache. These headache attacks occurred over periods lasting 2 to 3 weeks, separated by pain-free periods lasting 6 months or longer. There was no history of neck trauma or surgery. The patient visited his nearest hospital and was started on nortriptyline, which was not effective at preventing the headaches; however, they did respond to acetaminophen. He underwent brain magnetic resonance (MR) imaging, which produced normal findings. However, computed tomography (CT) angiography of the head and neck demonstrated an arteriovenous fistula between the left external carotid artery and the left external jugular vein (Fig. 1A). He visited our hospital for a second opinion, where he underwent conventional angiography, which confirmed the fistula (Fig. 1B and C). Coil embolization was performed, and the final conventional angiography showed no residual filling of the fistula (Fig. 1D). He was followed up for 2.5 years, during which he was free of exercise-induced and coital headaches. Most arteriovenous fistulas in the head and neck region occur as a result of trauma, iatrogenic injury, or extensive infection of the neck. Congenital arteriovenous fistulas between the external carotid artery and jugular vein are rare, and they are characterized by symptoms and signs such as pulsatile mass, pulsatile tinnitus, facial pain, vertigo, and dyspnea.2,3 It is not clear why the carotid–jugular fistula caused the exercise headaches in the present case. Halbach et al.4 investigated six patients with arteriovenous fistulas of the internal maxillary artery, and found that the most common initial symptom was bruit, which was exacerbated by exercise. Two theories on the pathophysiology of secondary exercise headache in our patient may be proposed. First, increased blood pressure during exercise may result in venous or arterial distension, which may cause engorgement of the arteriovenous fistula and mechanical compression of adjacent pain-sensitive structures.4,5 Second, increased intra-abdominal and intrathoracic pressures during exercise may be transmitted through the venous system into an Kyusik Kang Jae Hoon Kim Byung-Kun Kim","PeriodicalId":324902,"journal":{"name":"Journal of Clinical Neurology (Seoul, Korea)","volume":" ","pages":"93-95"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1c/b5/jcn-18-93.PMC8762513.pdf","citationCount":"1","resultStr":"{\"title\":\"Exercise Headache Associated With an Arteriovenous Fistula of the External Carotid Artery.\",\"authors\":\"Kyusik Kang, Jae Hoon Kim, Byung-Kun Kim\",\"doi\":\"10.3988/jcn.2022.18.1.93\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Dear Editor, Exercise headache is a headache provoked by exercise or exertion.1 Symptomatic causes of exercise headache include subarachnoid hemorrhage, arterial dissection, reversible cerebral vasoconstriction syndrome, and, less commonly, space-occupying lesions, sinusitis, Chiari malformation, and pheochromocytoma.1 We report a patient with recurrent exercise-induced and coital headaches associated with an arteriovenous fistula between the external carotid artery and the external jugular vein. A 27-year old male presented with a 15-year history of severe left occipital headaches induced by physical exercise (e.g., anaerobic leg exercises at a gym) and a 3-year history of headaches during coitus. The exercise-induced headaches peaked within 10 minutes, and then subsided over a couple of hours. He described a left occipital throbbing without associated nausea or light or noise sensitivity. The intensity was 8/10 at about 10 minutes after the onset. The headaches during coitus increased with the degree of sexual excitement. Coughing and other Valsalva (straining) maneuvers did not provoke the headache. These headache attacks occurred over periods lasting 2 to 3 weeks, separated by pain-free periods lasting 6 months or longer. There was no history of neck trauma or surgery. The patient visited his nearest hospital and was started on nortriptyline, which was not effective at preventing the headaches; however, they did respond to acetaminophen. He underwent brain magnetic resonance (MR) imaging, which produced normal findings. However, computed tomography (CT) angiography of the head and neck demonstrated an arteriovenous fistula between the left external carotid artery and the left external jugular vein (Fig. 1A). He visited our hospital for a second opinion, where he underwent conventional angiography, which confirmed the fistula (Fig. 1B and C). Coil embolization was performed, and the final conventional angiography showed no residual filling of the fistula (Fig. 1D). He was followed up for 2.5 years, during which he was free of exercise-induced and coital headaches. Most arteriovenous fistulas in the head and neck region occur as a result of trauma, iatrogenic injury, or extensive infection of the neck. Congenital arteriovenous fistulas between the external carotid artery and jugular vein are rare, and they are characterized by symptoms and signs such as pulsatile mass, pulsatile tinnitus, facial pain, vertigo, and dyspnea.2,3 It is not clear why the carotid–jugular fistula caused the exercise headaches in the present case. Halbach et al.4 investigated six patients with arteriovenous fistulas of the internal maxillary artery, and found that the most common initial symptom was bruit, which was exacerbated by exercise. Two theories on the pathophysiology of secondary exercise headache in our patient may be proposed. First, increased blood pressure during exercise may result in venous or arterial distension, which may cause engorgement of the arteriovenous fistula and mechanical compression of adjacent pain-sensitive structures.4,5 Second, increased intra-abdominal and intrathoracic pressures during exercise may be transmitted through the venous system into an Kyusik Kang Jae Hoon Kim Byung-Kun Kim\",\"PeriodicalId\":324902,\"journal\":{\"name\":\"Journal of Clinical Neurology (Seoul, Korea)\",\"volume\":\" \",\"pages\":\"93-95\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1c/b5/jcn-18-93.PMC8762513.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Neurology (Seoul, Korea)\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3988/jcn.2022.18.1.93\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Neurology (Seoul, Korea)","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3988/jcn.2022.18.1.93","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Exercise Headache Associated With an Arteriovenous Fistula of the External Carotid Artery.
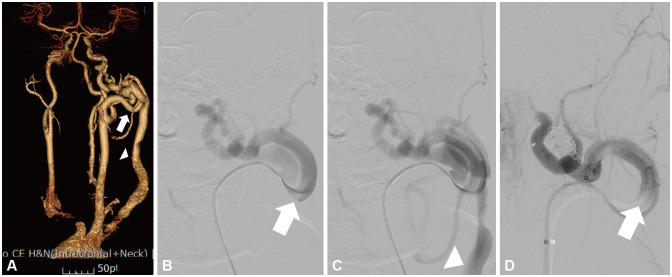
Dear Editor, Exercise headache is a headache provoked by exercise or exertion.1 Symptomatic causes of exercise headache include subarachnoid hemorrhage, arterial dissection, reversible cerebral vasoconstriction syndrome, and, less commonly, space-occupying lesions, sinusitis, Chiari malformation, and pheochromocytoma.1 We report a patient with recurrent exercise-induced and coital headaches associated with an arteriovenous fistula between the external carotid artery and the external jugular vein. A 27-year old male presented with a 15-year history of severe left occipital headaches induced by physical exercise (e.g., anaerobic leg exercises at a gym) and a 3-year history of headaches during coitus. The exercise-induced headaches peaked within 10 minutes, and then subsided over a couple of hours. He described a left occipital throbbing without associated nausea or light or noise sensitivity. The intensity was 8/10 at about 10 minutes after the onset. The headaches during coitus increased with the degree of sexual excitement. Coughing and other Valsalva (straining) maneuvers did not provoke the headache. These headache attacks occurred over periods lasting 2 to 3 weeks, separated by pain-free periods lasting 6 months or longer. There was no history of neck trauma or surgery. The patient visited his nearest hospital and was started on nortriptyline, which was not effective at preventing the headaches; however, they did respond to acetaminophen. He underwent brain magnetic resonance (MR) imaging, which produced normal findings. However, computed tomography (CT) angiography of the head and neck demonstrated an arteriovenous fistula between the left external carotid artery and the left external jugular vein (Fig. 1A). He visited our hospital for a second opinion, where he underwent conventional angiography, which confirmed the fistula (Fig. 1B and C). Coil embolization was performed, and the final conventional angiography showed no residual filling of the fistula (Fig. 1D). He was followed up for 2.5 years, during which he was free of exercise-induced and coital headaches. Most arteriovenous fistulas in the head and neck region occur as a result of trauma, iatrogenic injury, or extensive infection of the neck. Congenital arteriovenous fistulas between the external carotid artery and jugular vein are rare, and they are characterized by symptoms and signs such as pulsatile mass, pulsatile tinnitus, facial pain, vertigo, and dyspnea.2,3 It is not clear why the carotid–jugular fistula caused the exercise headaches in the present case. Halbach et al.4 investigated six patients with arteriovenous fistulas of the internal maxillary artery, and found that the most common initial symptom was bruit, which was exacerbated by exercise. Two theories on the pathophysiology of secondary exercise headache in our patient may be proposed. First, increased blood pressure during exercise may result in venous or arterial distension, which may cause engorgement of the arteriovenous fistula and mechanical compression of adjacent pain-sensitive structures.4,5 Second, increased intra-abdominal and intrathoracic pressures during exercise may be transmitted through the venous system into an Kyusik Kang Jae Hoon Kim Byung-Kun Kim

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


