Wi-Sun Ryu, Keun-Sik Hong, Sang-Wuk Jeong, Jung E Park, Beom Joon Kim, Joon-Tae Kim, Kyung Bok Lee, Tai Hwan Park, Sang-Soon Park, Jong-Moo Park, Kyusik Kang, Yong-Jin Cho, Hong-Kyun Park, Byung-Chul Lee, Kyung-Ho Yu, Mi Sun Oh, Soo Joo Lee, Jae Guk Kim, Jae-Kwan Cha, Dae-Hyun Kim, Jun Lee, Moon-Ku Han, Man Seok Park, Kang-Ho Choi, Juneyoung Lee, Jeffrey L Saver, Eng H Lo, Hee-Joon Bae, Dong-Eog Kim
{"title":"缺血性脑卒中发病时间与表现严重程度、急性进展和长期结果的关联:一项队列研究。","authors":"Wi-Sun Ryu, Keun-Sik Hong, Sang-Wuk Jeong, Jung E Park, Beom Joon Kim, Joon-Tae Kim, Kyung Bok Lee, Tai Hwan Park, Sang-Soon Park, Jong-Moo Park, Kyusik Kang, Yong-Jin Cho, Hong-Kyun Park, Byung-Chul Lee, Kyung-Ho Yu, Mi Sun Oh, Soo Joo Lee, Jae Guk Kim, Jae-Kwan Cha, Dae-Hyun Kim, Jun Lee, Moon-Ku Han, Man Seok Park, Kang-Ho Choi, Juneyoung Lee, Jeffrey L Saver, Eng H Lo, Hee-Joon Bae, Dong-Eog Kim","doi":"10.1371/journal.pmed.1003910","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Preclinical data suggest circadian variation in ischemic stroke progression, with more active cell death and infarct growth in rodent models with inactive phase (daytime) than active phase (nighttime) stroke onset. We aimed to examine the association of stroke onset time with presenting severity, early neurological deterioration (END), and long-term functional outcome in human ischemic stroke.</p><p><strong>Methods and findings: </strong>In a Korean nationwide multicenter observational cohort study from May 2011 to July 2020, we assessed circadian effects on initial stroke severity (National Institutes of Health Stroke Scale [NIHSS] score at admission), END, and favorable functional outcome (3-month modified Rankin Scale [mRS] score 0 to 2 versus 3 to 6). We included 17,461 consecutive patients with witnessed ischemic stroke within 6 hours of onset. Stroke onset time was divided into 2 groups (day-onset [06:00 to 18:00] versus night-onset [18:00 to 06:00]) and into 6 groups by 4-hour intervals. We used mixed-effects ordered or logistic regression models while accounting for clustering by hospitals. Mean age was 66.9 (SD 13.4) years, and 6,900 (39.5%) were women. END occurred in 2,219 (12.7%) patients. After adjusting for covariates including age, sex, previous stroke, prestroke mRS score, admission NIHSS score, hypertension, diabetes, hyperlipidemia, smoking, atrial fibrillation, prestroke antiplatelet use, prestroke statin use, revascularization, season of stroke onset, and time from onset to hospital arrival, night-onset stroke was more prone to END (adjusted incidence 14.4% versus 12.8%, p = 0.006) and had a lower likelihood of favorable outcome (adjusted odds ratio, 0.88 [95% CI, 0.79 to 0.98]; p = 0.03) compared with day-onset stroke. When stroke onset times were grouped by 4-hour intervals, a monotonic gradient in presenting NIHSS score was noted, rising from a nadir in 06:00 to 10:00 to a peak in 02:00 to 06:00. The 18:00 to 22:00 and 22:00 to 02:00 onset stroke patients were more likely to experience END than the 06:00 to 10:00 onset stroke patients. At 3 months, there was a monotonic gradient in the rate of favorable functional outcome, falling from a peak at 06:00 to 10:00 to a nadir at 22:00 to 02:00. Study limitations include the lack of information on sleep disorders and patient work/activity schedules.</p><p><strong>Conclusions: </strong>Night-onset strokes, compared with day-onset strokes, are associated with higher presenting neurologic severity, more frequent END, and worse 3-month functional outcome. These findings suggest that circadian time of onset is an important additional variable for inclusion in epidemiologic natural history studies and in treatment trials of neuroprotective and reperfusion agents for acute ischemic stroke.</p>","PeriodicalId":20368,"journal":{"name":"PLoS Medicine","volume":"19 2","pages":"e1003910"},"PeriodicalIF":10.5000,"publicationDate":"2022-02-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8815976/pdf/","citationCount":"23","resultStr":"{\"title\":\"Association of ischemic stroke onset time with presenting severity, acute progression, and long-term outcome: A cohort study.\",\"authors\":\"Wi-Sun Ryu, Keun-Sik Hong, Sang-Wuk Jeong, Jung E Park, Beom Joon Kim, Joon-Tae Kim, Kyung Bok Lee, Tai Hwan Park, Sang-Soon Park, Jong-Moo Park, Kyusik Kang, Yong-Jin Cho, Hong-Kyun Park, Byung-Chul Lee, Kyung-Ho Yu, Mi Sun Oh, Soo Joo Lee, Jae Guk Kim, Jae-Kwan Cha, Dae-Hyun Kim, Jun Lee, Moon-Ku Han, Man Seok Park, Kang-Ho Choi, Juneyoung Lee, Jeffrey L Saver, Eng H Lo, Hee-Joon Bae, Dong-Eog Kim\",\"doi\":\"10.1371/journal.pmed.1003910\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Preclinical data suggest circadian variation in ischemic stroke progression, with more active cell death and infarct growth in rodent models with inactive phase (daytime) than active phase (nighttime) stroke onset. We aimed to examine the association of stroke onset time with presenting severity, early neurological deterioration (END), and long-term functional outcome in human ischemic stroke.</p><p><strong>Methods and findings: </strong>In a Korean nationwide multicenter observational cohort study from May 2011 to July 2020, we assessed circadian effects on initial stroke severity (National Institutes of Health Stroke Scale [NIHSS] score at admission), END, and favorable functional outcome (3-month modified Rankin Scale [mRS] score 0 to 2 versus 3 to 6). We included 17,461 consecutive patients with witnessed ischemic stroke within 6 hours of onset. Stroke onset time was divided into 2 groups (day-onset [06:00 to 18:00] versus night-onset [18:00 to 06:00]) and into 6 groups by 4-hour intervals. We used mixed-effects ordered or logistic regression models while accounting for clustering by hospitals. Mean age was 66.9 (SD 13.4) years, and 6,900 (39.5%) were women. END occurred in 2,219 (12.7%) patients. After adjusting for covariates including age, sex, previous stroke, prestroke mRS score, admission NIHSS score, hypertension, diabetes, hyperlipidemia, smoking, atrial fibrillation, prestroke antiplatelet use, prestroke statin use, revascularization, season of stroke onset, and time from onset to hospital arrival, night-onset stroke was more prone to END (adjusted incidence 14.4% versus 12.8%, p = 0.006) and had a lower likelihood of favorable outcome (adjusted odds ratio, 0.88 [95% CI, 0.79 to 0.98]; p = 0.03) compared with day-onset stroke. When stroke onset times were grouped by 4-hour intervals, a monotonic gradient in presenting NIHSS score was noted, rising from a nadir in 06:00 to 10:00 to a peak in 02:00 to 06:00. The 18:00 to 22:00 and 22:00 to 02:00 onset stroke patients were more likely to experience END than the 06:00 to 10:00 onset stroke patients. At 3 months, there was a monotonic gradient in the rate of favorable functional outcome, falling from a peak at 06:00 to 10:00 to a nadir at 22:00 to 02:00. Study limitations include the lack of information on sleep disorders and patient work/activity schedules.</p><p><strong>Conclusions: </strong>Night-onset strokes, compared with day-onset strokes, are associated with higher presenting neurologic severity, more frequent END, and worse 3-month functional outcome. These findings suggest that circadian time of onset is an important additional variable for inclusion in epidemiologic natural history studies and in treatment trials of neuroprotective and reperfusion agents for acute ischemic stroke.</p>\",\"PeriodicalId\":20368,\"journal\":{\"name\":\"PLoS Medicine\",\"volume\":\"19 2\",\"pages\":\"e1003910\"},\"PeriodicalIF\":10.5000,\"publicationDate\":\"2022-02-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8815976/pdf/\",\"citationCount\":\"23\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PLoS Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1371/journal.pmed.1003910\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/2/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1371/journal.pmed.1003910","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/2/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Association of ischemic stroke onset time with presenting severity, acute progression, and long-term outcome: A cohort study.
Background: Preclinical data suggest circadian variation in ischemic stroke progression, with more active cell death and infarct growth in rodent models with inactive phase (daytime) than active phase (nighttime) stroke onset. We aimed to examine the association of stroke onset time with presenting severity, early neurological deterioration (END), and long-term functional outcome in human ischemic stroke.
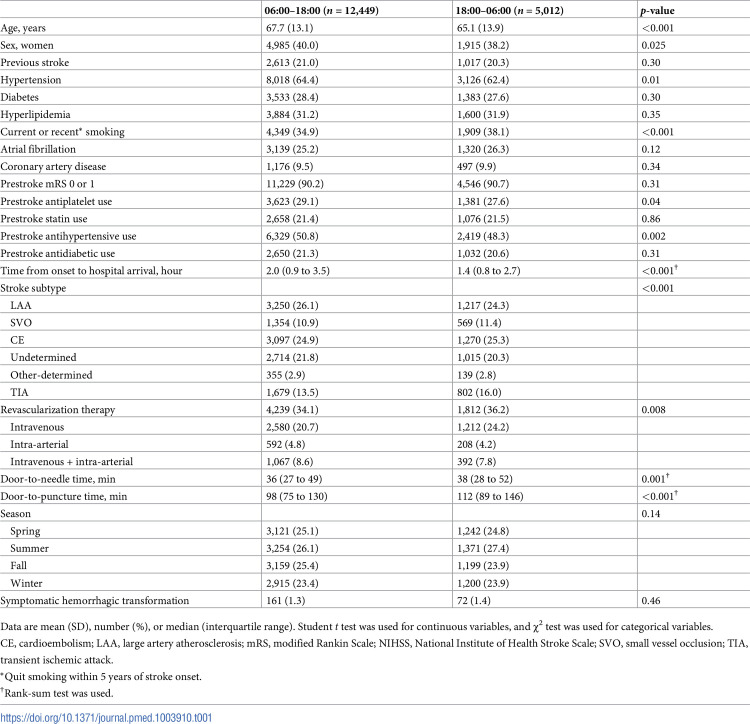
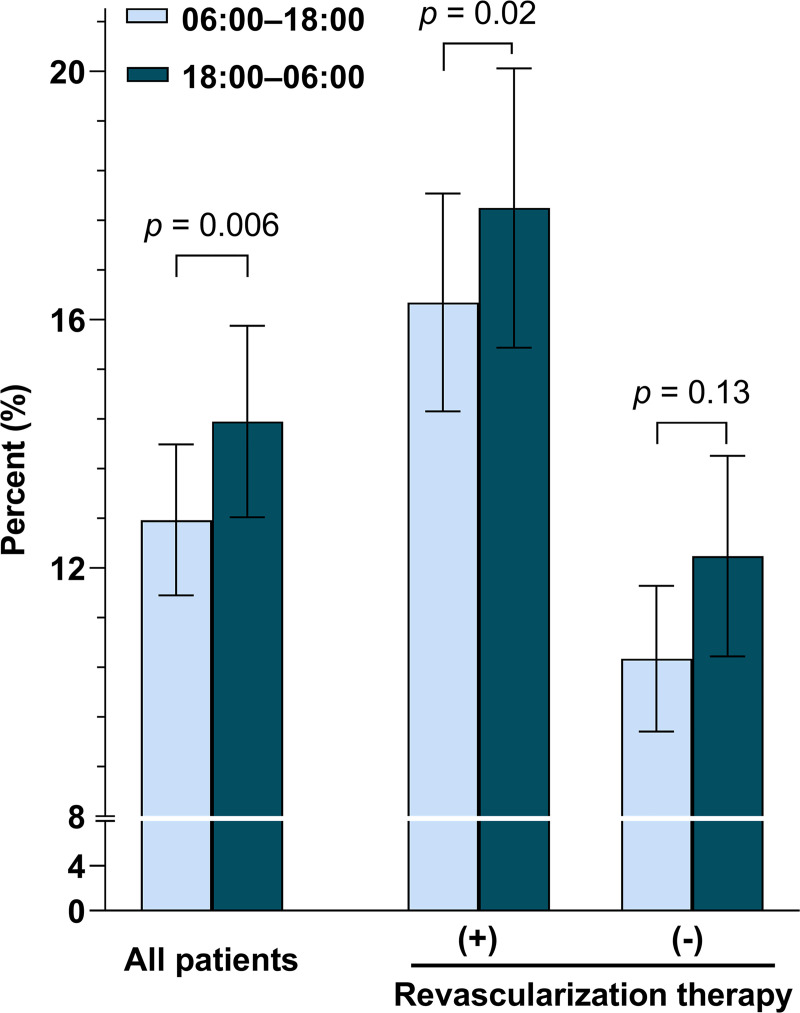
Methods and findings: In a Korean nationwide multicenter observational cohort study from May 2011 to July 2020, we assessed circadian effects on initial stroke severity (National Institutes of Health Stroke Scale [NIHSS] score at admission), END, and favorable functional outcome (3-month modified Rankin Scale [mRS] score 0 to 2 versus 3 to 6). We included 17,461 consecutive patients with witnessed ischemic stroke within 6 hours of onset. Stroke onset time was divided into 2 groups (day-onset [06:00 to 18:00] versus night-onset [18:00 to 06:00]) and into 6 groups by 4-hour intervals. We used mixed-effects ordered or logistic regression models while accounting for clustering by hospitals. Mean age was 66.9 (SD 13.4) years, and 6,900 (39.5%) were women. END occurred in 2,219 (12.7%) patients. After adjusting for covariates including age, sex, previous stroke, prestroke mRS score, admission NIHSS score, hypertension, diabetes, hyperlipidemia, smoking, atrial fibrillation, prestroke antiplatelet use, prestroke statin use, revascularization, season of stroke onset, and time from onset to hospital arrival, night-onset stroke was more prone to END (adjusted incidence 14.4% versus 12.8%, p = 0.006) and had a lower likelihood of favorable outcome (adjusted odds ratio, 0.88 [95% CI, 0.79 to 0.98]; p = 0.03) compared with day-onset stroke. When stroke onset times were grouped by 4-hour intervals, a monotonic gradient in presenting NIHSS score was noted, rising from a nadir in 06:00 to 10:00 to a peak in 02:00 to 06:00. The 18:00 to 22:00 and 22:00 to 02:00 onset stroke patients were more likely to experience END than the 06:00 to 10:00 onset stroke patients. At 3 months, there was a monotonic gradient in the rate of favorable functional outcome, falling from a peak at 06:00 to 10:00 to a nadir at 22:00 to 02:00. Study limitations include the lack of information on sleep disorders and patient work/activity schedules.
Conclusions: Night-onset strokes, compared with day-onset strokes, are associated with higher presenting neurologic severity, more frequent END, and worse 3-month functional outcome. These findings suggest that circadian time of onset is an important additional variable for inclusion in epidemiologic natural history studies and in treatment trials of neuroprotective and reperfusion agents for acute ischemic stroke.
期刊介绍:
PLOS Medicine aims to be a leading platform for research and analysis on the global health challenges faced by humanity. The journal covers a wide range of topics, including biomedicine, the environment, society, and politics, that affect the well-being of individuals worldwide. It particularly highlights studies that contribute to clinical practice, health policy, or our understanding of disease mechanisms, with the ultimate goal of improving health outcomes in diverse settings.
Unwavering in its commitment to ethical standards, PLOS Medicine ensures integrity in medical publishing. This includes actively managing and transparently disclosing any conflicts of interest during the reporting, peer review, and publication processes. The journal promotes transparency by providing visibility into the review and publication procedures. It also encourages data sharing and the reuse of published work. Author rights are upheld, allowing them to retain copyright. Furthermore, PLOS Medicine strongly supports Open Access publishing, making research articles freely available to all without restrictions, facilitating widespread dissemination of knowledge. The journal does not endorse drug or medical device advertising and refrains from exclusive sales of reprints to avoid conflicts of interest.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


