Erica A K Davis, Tyler Hightower, Katherine Ann Cinnamon
{"title":"毒性氯氮平水平是严重急性感染的第一指征。","authors":"Erica A K Davis, Tyler Hightower, Katherine Ann Cinnamon","doi":"10.9740/mhc.2022.01.045","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Clozapine levels can be influenced by many factors, including pharmacogenomic variability, pharmacokinetic drug interactions, and infection/inflammation. The concentration-to-dose ratio (C/D), a measure of a medication's rate of metabolism and clearance, may increase during an acute infection due to decreased medication metabolism and clearance.</p><p><strong>Case report: </strong>A 56-year-old White man was restarted on clozapine and titrated up to 350 mg/d with therapeutic steady-state levels (C/D 1.11) on hospital day (HD) 69. At this time, he was also being treated for COPD exacerbation. For the next month, he continued to complain of cough, but vital signs and chest x-ray remained normal. Labs were unremarkable except for occasional leukocytosis that would resolve on repeat evaluation. A routine clozapine level drawn on HD 104, resulted on day 108 and showed clozapine toxicity with C/D 4.05, although the patient was asymptomatic. After receipt of labs on day 109, showing elevated WBC count, he was immediately sent to the emergency room where he was admitted for treatment of pneumonia. On return to the state hospital, the patient was continued on 100 mg clozapine and titrated to 200 mg/d based on low drug levels. He continued to do well on 200 mg/d clozapine with C/D averaging 1.13 (range, 0.75-1.52).</p><p><strong>Discussion: </strong>Acute infection and illness can lead to significantly increased clozapine levels and toxicity, even if symptoms of toxicity are minimal or absent. This appears to be the first report of a toxic level being the first indication of severe medical illness.</p>","PeriodicalId":22710,"journal":{"name":"The Mental Health Clinician","volume":"12 1","pages":"45-48"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a6/38/i2168-9709-12-1-45.PMC8788300.pdf","citationCount":"0","resultStr":"{\"title\":\"Toxic clozapine level as first indication of severe, acute infection.\",\"authors\":\"Erica A K Davis, Tyler Hightower, Katherine Ann Cinnamon\",\"doi\":\"10.9740/mhc.2022.01.045\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Clozapine levels can be influenced by many factors, including pharmacogenomic variability, pharmacokinetic drug interactions, and infection/inflammation. The concentration-to-dose ratio (C/D), a measure of a medication's rate of metabolism and clearance, may increase during an acute infection due to decreased medication metabolism and clearance.</p><p><strong>Case report: </strong>A 56-year-old White man was restarted on clozapine and titrated up to 350 mg/d with therapeutic steady-state levels (C/D 1.11) on hospital day (HD) 69. At this time, he was also being treated for COPD exacerbation. For the next month, he continued to complain of cough, but vital signs and chest x-ray remained normal. Labs were unremarkable except for occasional leukocytosis that would resolve on repeat evaluation. A routine clozapine level drawn on HD 104, resulted on day 108 and showed clozapine toxicity with C/D 4.05, although the patient was asymptomatic. After receipt of labs on day 109, showing elevated WBC count, he was immediately sent to the emergency room where he was admitted for treatment of pneumonia. On return to the state hospital, the patient was continued on 100 mg clozapine and titrated to 200 mg/d based on low drug levels. He continued to do well on 200 mg/d clozapine with C/D averaging 1.13 (range, 0.75-1.52).</p><p><strong>Discussion: </strong>Acute infection and illness can lead to significantly increased clozapine levels and toxicity, even if symptoms of toxicity are minimal or absent. This appears to be the first report of a toxic level being the first indication of severe medical illness.</p>\",\"PeriodicalId\":22710,\"journal\":{\"name\":\"The Mental Health Clinician\",\"volume\":\"12 1\",\"pages\":\"45-48\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-01-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a6/38/i2168-9709-12-1-45.PMC8788300.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Mental Health Clinician\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.9740/mhc.2022.01.045\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Mental Health Clinician","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.9740/mhc.2022.01.045","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:氯氮平水平受多种因素影响,包括药物基因组变异性、药代动力学药物相互作用和感染/炎症。浓度剂量比(C/D)是衡量药物代谢和清除率的指标,在急性感染期间可能由于药物代谢和清除率降低而增加。病例报告:一名56岁白人男性在住院日(HD) 69重新开始使用氯氮平,并滴定至350mg /d,达到治疗稳态水平(C/ d 1.11)。此时,他也在接受慢性阻塞性肺病加重治疗。在接下来的一个月里,他一直抱怨咳嗽,但生命体征和胸部x光片都很正常。除偶尔出现白细胞增多外,实验室无明显异常,可在重复检查时消除。第108天HD 104的氯氮平常规水平显示氯氮平毒性,C/D为4.05,尽管患者无症状。在第109天收到化验单后,显示白细胞计数升高,他立即被送往急诊室接受肺炎治疗。返回州立医院后,患者继续服用100毫克氯氮平,并根据低药物水平滴定至200毫克/天。他继续服用200mg /d氯氮平,C/ d平均为1.13(范围为0.75-1.52)。讨论:急性感染和疾病可导致氯氮平水平和毒性显著增加,即使毒性症状很轻微或没有。这似乎是毒性水平作为严重医学疾病的第一个指征的第一个报告。
Toxic clozapine level as first indication of severe, acute infection.
Background: Clozapine levels can be influenced by many factors, including pharmacogenomic variability, pharmacokinetic drug interactions, and infection/inflammation. The concentration-to-dose ratio (C/D), a measure of a medication's rate of metabolism and clearance, may increase during an acute infection due to decreased medication metabolism and clearance.
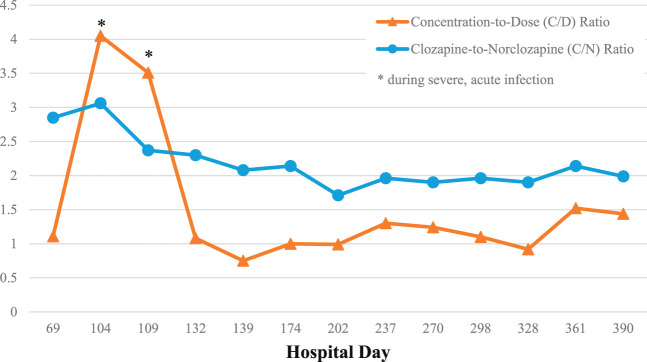
Case report: A 56-year-old White man was restarted on clozapine and titrated up to 350 mg/d with therapeutic steady-state levels (C/D 1.11) on hospital day (HD) 69. At this time, he was also being treated for COPD exacerbation. For the next month, he continued to complain of cough, but vital signs and chest x-ray remained normal. Labs were unremarkable except for occasional leukocytosis that would resolve on repeat evaluation. A routine clozapine level drawn on HD 104, resulted on day 108 and showed clozapine toxicity with C/D 4.05, although the patient was asymptomatic. After receipt of labs on day 109, showing elevated WBC count, he was immediately sent to the emergency room where he was admitted for treatment of pneumonia. On return to the state hospital, the patient was continued on 100 mg clozapine and titrated to 200 mg/d based on low drug levels. He continued to do well on 200 mg/d clozapine with C/D averaging 1.13 (range, 0.75-1.52).
Discussion: Acute infection and illness can lead to significantly increased clozapine levels and toxicity, even if symptoms of toxicity are minimal or absent. This appears to be the first report of a toxic level being the first indication of severe medical illness.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


