Katharina Doni, Stefanie Bühn, Alina Weise, Nina-Kristin Mann, Simone Hess, Andreas Sönnichsen, Dawid Pieper, Petra Thürmann, Tim Mathes
{"title":"二肽基肽酶-4抑制剂对老年2型糖尿病患者的安全性:随机对照试验的系统评价和荟萃分析","authors":"Katharina Doni, Stefanie Bühn, Alina Weise, Nina-Kristin Mann, Simone Hess, Andreas Sönnichsen, Dawid Pieper, Petra Thürmann, Tim Mathes","doi":"10.1177/20420986211072383","DOIUrl":null,"url":null,"abstract":"<p><strong>Registration: </strong>PROSPERO: CRD42020210645.</p><p><strong>Introduction: </strong>We aimed to assess the safety of dipeptidyl peptidase-4 (DPP-4) inhibitors in older patients with type 2 diabetes with inadequate glycaemic control.</p><p><strong>Methods: </strong>We included randomized controlled trials (RCTs) in older (⩾65 years) patients with type 2 diabetes. The intervention group was randomized to treatment with any DPP-4 inhibitors. A systematic search in MEDLINE and Embase was performed in December 2020. For assessing the risk of bias, RoB 2 tool was applied. The quality of evidence was assessed using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach. We pooled outcomes using random effects meta-analyses.</p><p><strong>Results: </strong>We identified 16 RCTs that included 19,317 patients with a mean age of greater than 70 years. The mean HbA1c level ranged between 7.1 and 10.0 g/dl. Adding DPP-4 inhibitors to standard care alone may increase mortality slightly [risk ratio (RR) 1.04; 95% confidence interval (CI) 0.89-1.21]. Adding DPP-4 inhibitors to standard care increases the risk for hypoglycaemia (RR 1.08; 95% CI 1.01-1.16), but difference in overall adverse events is negligible. DPP-4 inhibitors added to standard care may reduce mortality compared with sulfonylureas (RR 0.88; 95% CI 0.75-1.04). DPP-4 inhibitors probably reduce the risk for hypoglycaemia compared with sulfonylureas (magnitude of effect not quantifiable because of heterogeneity) but difference in overall adverse events is negligible. There is insufficient evidence on hospitalizations, falls, fractures, renal impairment and pancreatitis.</p><p><strong>Conclusion: </strong>There is no evidence that DPP-4 inhibitors in addition to standard care decrease mortality but DPP-4 inhibitors increase hypoglycaemia risk. Second-line therapy in older patients should be considered cautiously even in drugs with a good safety profile such as DPP-4 inhibitors. In case second-line treatment is necessary, DPP-4 inhibitors appear to be preferable to sulfonylureas.</p><p><strong>Plain language summary: </strong><b>Safety of dipeptidyl peptidase-4 inhibitors in older adults with type 2 diabetes:</b> <b>Introduction::</b> We performed the review to assess the safety of dipeptidyl peptidase-4 (DPP-4) inhibitors in older type 2 diabetes patients with blood sugar outside the normal level.<b>Methods::</b> To answer the question, we searched various electronic databases. We included studies in older (⩾65 years) patients with type 2 diabetes that assessed the safety of DPP-4 inhibitors. The data from the different studies were quantitatively summarized using statistical methods. We assessed the quality of the data to judge the certainty of the findings.<b>Results::</b> We identified 16 studies that included 19,317 patients with a mean age greater than 70 years. The average blood sugar level of patients in the included studies was slightly or moderately increased. Adding DPP-4 inhibitors to standard care alone may increase mortality slightly. Adding DPP-4 inhibitors to standard care increases the risk for hypoglycaemia, but difference in overall adverse events is negligible. DPP-4 inhibitors added to standard care may reduce mortality compared with sulfonylureas. DPP-4s probably reduce the risk of hypoglycaemia compared with sulfonylureas (magnitude of effect not quantifiable because of heterogeneity) but difference in overall adverse events is negligible. There is insufficient evidence on hospitalizations, falls, fractures, renal impairment and pancreatitis.<b>Conclusion::</b> There is no evidence that DPP-4 inhibitors in addition to standard care decrease mortality but DPP-4 inhibitors increase the risk that blood sugar falls below normal. Adding DPP-4 inhibitorss to standard care in older patients should be considered cautiously even in drugs with a good safety profile such as DPP-4 inhibitors. In case additional treatment is necessary, DPP-4 inhibitors appear to be preferable to sulfonylureas.</p>","PeriodicalId":23012,"journal":{"name":"Therapeutic Advances in Drug Safety","volume":" ","pages":"20420986211072383"},"PeriodicalIF":3.4000,"publicationDate":"2022-01-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8785305/pdf/","citationCount":"4","resultStr":"{\"title\":\"Safety of dipeptidyl peptidase-4 inhibitors in older adults with type 2 diabetes: a systematic review and meta-analysis of randomized controlled trials.\",\"authors\":\"Katharina Doni, Stefanie Bühn, Alina Weise, Nina-Kristin Mann, Simone Hess, Andreas Sönnichsen, Dawid Pieper, Petra Thürmann, Tim Mathes\",\"doi\":\"10.1177/20420986211072383\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Registration: </strong>PROSPERO: CRD42020210645.</p><p><strong>Introduction: </strong>We aimed to assess the safety of dipeptidyl peptidase-4 (DPP-4) inhibitors in older patients with type 2 diabetes with inadequate glycaemic control.</p><p><strong>Methods: </strong>We included randomized controlled trials (RCTs) in older (⩾65 years) patients with type 2 diabetes. The intervention group was randomized to treatment with any DPP-4 inhibitors. A systematic search in MEDLINE and Embase was performed in December 2020. For assessing the risk of bias, RoB 2 tool was applied. The quality of evidence was assessed using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach. We pooled outcomes using random effects meta-analyses.</p><p><strong>Results: </strong>We identified 16 RCTs that included 19,317 patients with a mean age of greater than 70 years. The mean HbA1c level ranged between 7.1 and 10.0 g/dl. Adding DPP-4 inhibitors to standard care alone may increase mortality slightly [risk ratio (RR) 1.04; 95% confidence interval (CI) 0.89-1.21]. Adding DPP-4 inhibitors to standard care increases the risk for hypoglycaemia (RR 1.08; 95% CI 1.01-1.16), but difference in overall adverse events is negligible. DPP-4 inhibitors added to standard care may reduce mortality compared with sulfonylureas (RR 0.88; 95% CI 0.75-1.04). DPP-4 inhibitors probably reduce the risk for hypoglycaemia compared with sulfonylureas (magnitude of effect not quantifiable because of heterogeneity) but difference in overall adverse events is negligible. There is insufficient evidence on hospitalizations, falls, fractures, renal impairment and pancreatitis.</p><p><strong>Conclusion: </strong>There is no evidence that DPP-4 inhibitors in addition to standard care decrease mortality but DPP-4 inhibitors increase hypoglycaemia risk. Second-line therapy in older patients should be considered cautiously even in drugs with a good safety profile such as DPP-4 inhibitors. In case second-line treatment is necessary, DPP-4 inhibitors appear to be preferable to sulfonylureas.</p><p><strong>Plain language summary: </strong><b>Safety of dipeptidyl peptidase-4 inhibitors in older adults with type 2 diabetes:</b> <b>Introduction::</b> We performed the review to assess the safety of dipeptidyl peptidase-4 (DPP-4) inhibitors in older type 2 diabetes patients with blood sugar outside the normal level.<b>Methods::</b> To answer the question, we searched various electronic databases. We included studies in older (⩾65 years) patients with type 2 diabetes that assessed the safety of DPP-4 inhibitors. The data from the different studies were quantitatively summarized using statistical methods. We assessed the quality of the data to judge the certainty of the findings.<b>Results::</b> We identified 16 studies that included 19,317 patients with a mean age greater than 70 years. The average blood sugar level of patients in the included studies was slightly or moderately increased. Adding DPP-4 inhibitors to standard care alone may increase mortality slightly. Adding DPP-4 inhibitors to standard care increases the risk for hypoglycaemia, but difference in overall adverse events is negligible. DPP-4 inhibitors added to standard care may reduce mortality compared with sulfonylureas. DPP-4s probably reduce the risk of hypoglycaemia compared with sulfonylureas (magnitude of effect not quantifiable because of heterogeneity) but difference in overall adverse events is negligible. There is insufficient evidence on hospitalizations, falls, fractures, renal impairment and pancreatitis.<b>Conclusion::</b> There is no evidence that DPP-4 inhibitors in addition to standard care decrease mortality but DPP-4 inhibitors increase the risk that blood sugar falls below normal. Adding DPP-4 inhibitorss to standard care in older patients should be considered cautiously even in drugs with a good safety profile such as DPP-4 inhibitors. In case additional treatment is necessary, DPP-4 inhibitors appear to be preferable to sulfonylureas.</p>\",\"PeriodicalId\":23012,\"journal\":{\"name\":\"Therapeutic Advances in Drug Safety\",\"volume\":\" \",\"pages\":\"20420986211072383\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2022-01-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8785305/pdf/\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Drug Safety\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/20420986211072383\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Drug Safety","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/20420986211072383","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 4
摘要
注册号:PROSPERO: CRD42020210645。前言:我们旨在评估二肽基肽酶-4 (DPP-4)抑制剂在血糖控制不佳的老年2型糖尿病患者中的安全性。方法:我们在老年(大于或等于65岁)2型糖尿病患者中纳入了随机对照试验(rct)。干预组随机接受任意DPP-4抑制剂治疗。于2020年12月在MEDLINE和Embase中进行了系统检索。为评估偏倚风险,采用RoB 2工具。采用推荐、评估、发展和评价分级(GRADE)方法评估证据质量。我们使用随机效应荟萃分析汇总结果。结果:我们确定了16项随机对照试验,包括19317例平均年龄大于70岁的患者。平均HbA1c水平在7.1 - 10.0 g/dl之间。在标准治疗中单独加入DPP-4抑制剂可能会略微增加死亡率[危险比(RR) 1.04;95%置信区间(CI) 0.89-1.21]。在标准治疗中加入DPP-4抑制剂会增加低血糖的风险(RR 1.08;95% CI 1.01-1.16),但总体不良事件的差异可以忽略不计。与磺脲类药物相比,标准治疗中加入DPP-4抑制剂可降低死亡率(RR 0.88;95% ci 0.75-1.04)。与磺脲类药物相比,DPP-4抑制剂可能降低低血糖的风险(由于异质性,影响程度无法量化),但总体不良事件的差异可以忽略不计。关于住院、跌倒、骨折、肾功能损害和胰腺炎的证据不足。结论:没有证据表明DPP-4抑制剂在标准治疗之外可以降低死亡率,但DPP-4抑制剂会增加低血糖风险。老年患者的二线治疗应谨慎考虑,即使是具有良好安全性的药物,如DPP-4抑制剂。如果需要二线治疗,DPP-4抑制剂似乎比磺脲类药物更可取。摘要:二肽基肽酶-4抑制剂在老年2型糖尿病患者中的安全性:简介:我们进行了这项综述,以评估二肽基肽酶-4 (DPP-4)抑制剂在血糖高于正常水平的老年2型糖尿病患者中的安全性。方法:为了回答这个问题,我们检索了各种电子数据库。我们纳入了对年龄较大(小于65岁)的2型糖尿病患者的研究,评估了DPP-4抑制剂的安全性。采用统计学方法对不同研究的数据进行定量总结。我们评估了数据的质量,以判断研究结果的确定性。结果:我们确定了16项研究,包括19317例平均年龄大于70岁的患者。在纳入的研究中,患者的平均血糖水平有轻微或中度升高。在标准治疗中单独加入DPP-4抑制剂可能会略微增加死亡率。在标准治疗中加入DPP-4抑制剂会增加低血糖的风险,但总体不良事件的差异可以忽略不计。与磺脲类药物相比,标准治疗中加入DPP-4抑制剂可降低死亡率。与磺脲类药物相比,dpp -4可能降低低血糖的风险(由于异质性,影响程度无法量化),但总体不良事件的差异可以忽略不计。关于住院、跌倒、骨折、肾功能损害和胰腺炎的证据不足。结论:没有证据表明DPP-4抑制剂在标准治疗之外可以降低死亡率,但DPP-4抑制剂会增加血糖低于正常水平的风险。在老年患者的标准治疗中加入DPP-4抑制剂应谨慎考虑,即使是使用具有良好安全性的药物,如DPP-4抑制剂。如果需要额外的治疗,DPP-4抑制剂似乎比磺脲类药物更可取。
Safety of dipeptidyl peptidase-4 inhibitors in older adults with type 2 diabetes: a systematic review and meta-analysis of randomized controlled trials.
Registration: PROSPERO: CRD42020210645.
Introduction: We aimed to assess the safety of dipeptidyl peptidase-4 (DPP-4) inhibitors in older patients with type 2 diabetes with inadequate glycaemic control.
Methods: We included randomized controlled trials (RCTs) in older (⩾65 years) patients with type 2 diabetes. The intervention group was randomized to treatment with any DPP-4 inhibitors. A systematic search in MEDLINE and Embase was performed in December 2020. For assessing the risk of bias, RoB 2 tool was applied. The quality of evidence was assessed using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach. We pooled outcomes using random effects meta-analyses.
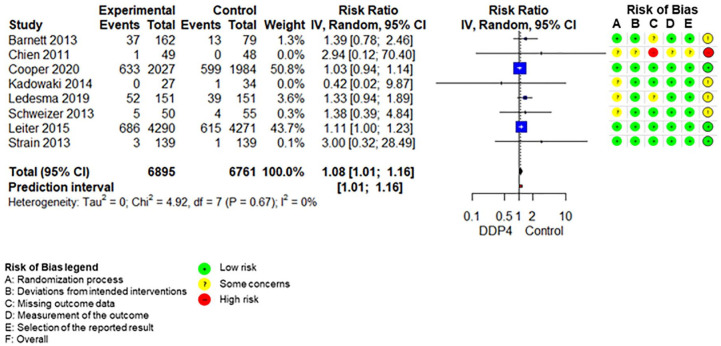
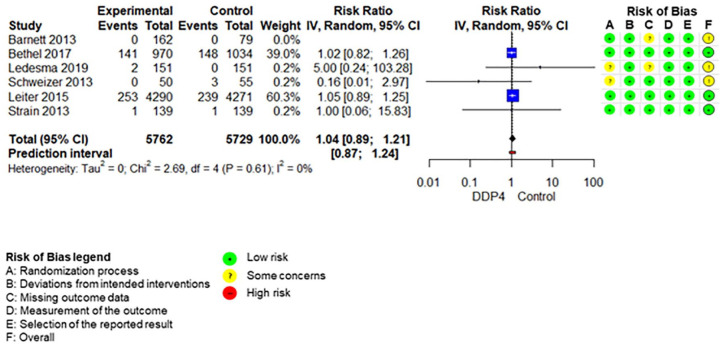
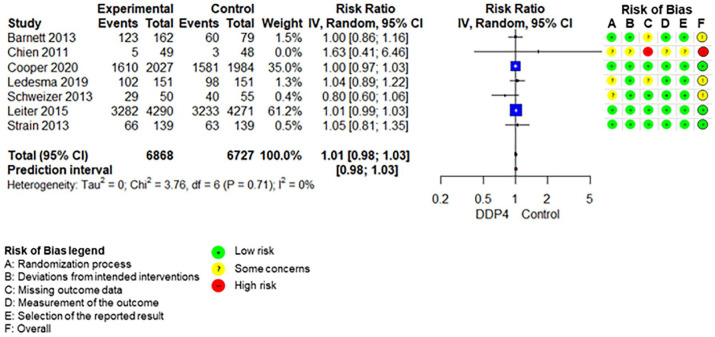
Results: We identified 16 RCTs that included 19,317 patients with a mean age of greater than 70 years. The mean HbA1c level ranged between 7.1 and 10.0 g/dl. Adding DPP-4 inhibitors to standard care alone may increase mortality slightly [risk ratio (RR) 1.04; 95% confidence interval (CI) 0.89-1.21]. Adding DPP-4 inhibitors to standard care increases the risk for hypoglycaemia (RR 1.08; 95% CI 1.01-1.16), but difference in overall adverse events is negligible. DPP-4 inhibitors added to standard care may reduce mortality compared with sulfonylureas (RR 0.88; 95% CI 0.75-1.04). DPP-4 inhibitors probably reduce the risk for hypoglycaemia compared with sulfonylureas (magnitude of effect not quantifiable because of heterogeneity) but difference in overall adverse events is negligible. There is insufficient evidence on hospitalizations, falls, fractures, renal impairment and pancreatitis.
Conclusion: There is no evidence that DPP-4 inhibitors in addition to standard care decrease mortality but DPP-4 inhibitors increase hypoglycaemia risk. Second-line therapy in older patients should be considered cautiously even in drugs with a good safety profile such as DPP-4 inhibitors. In case second-line treatment is necessary, DPP-4 inhibitors appear to be preferable to sulfonylureas.
Plain language summary: Safety of dipeptidyl peptidase-4 inhibitors in older adults with type 2 diabetes:Introduction:: We performed the review to assess the safety of dipeptidyl peptidase-4 (DPP-4) inhibitors in older type 2 diabetes patients with blood sugar outside the normal level.Methods:: To answer the question, we searched various electronic databases. We included studies in older (⩾65 years) patients with type 2 diabetes that assessed the safety of DPP-4 inhibitors. The data from the different studies were quantitatively summarized using statistical methods. We assessed the quality of the data to judge the certainty of the findings.Results:: We identified 16 studies that included 19,317 patients with a mean age greater than 70 years. The average blood sugar level of patients in the included studies was slightly or moderately increased. Adding DPP-4 inhibitors to standard care alone may increase mortality slightly. Adding DPP-4 inhibitors to standard care increases the risk for hypoglycaemia, but difference in overall adverse events is negligible. DPP-4 inhibitors added to standard care may reduce mortality compared with sulfonylureas. DPP-4s probably reduce the risk of hypoglycaemia compared with sulfonylureas (magnitude of effect not quantifiable because of heterogeneity) but difference in overall adverse events is negligible. There is insufficient evidence on hospitalizations, falls, fractures, renal impairment and pancreatitis.Conclusion:: There is no evidence that DPP-4 inhibitors in addition to standard care decrease mortality but DPP-4 inhibitors increase the risk that blood sugar falls below normal. Adding DPP-4 inhibitorss to standard care in older patients should be considered cautiously even in drugs with a good safety profile such as DPP-4 inhibitors. In case additional treatment is necessary, DPP-4 inhibitors appear to be preferable to sulfonylureas.
期刊介绍:
Therapeutic Advances in Drug Safety delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies pertaining to the safe use of drugs in patients.
The journal has a strong clinical and pharmacological focus and is aimed at clinicians and researchers in drug safety, providing a forum in print and online for publishing the highest quality articles in this area. The editors welcome articles of current interest on research across all areas of drug safety, including therapeutic drug monitoring, pharmacoepidemiology, adverse drug reactions, drug interactions, pharmacokinetics, pharmacovigilance, medication/prescribing errors, risk management, ethics and regulation.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


