Kat S Rock, Ching-I Huang, Ronald E Crump, Paul R Bessell, Paul E Brown, Inaki Tirados, Philippe Solano, Marina Antillon, Albert Picado, Severin Mbainda, Justin Darnas, Emily H Crowley, Steve J Torr, Mallaye Peka
{"title":"乍得曼杜勒重点地区冈比亚非洲锥虫病传播模型和预测的更新。","authors":"Kat S Rock, Ching-I Huang, Ronald E Crump, Paul R Bessell, Paul E Brown, Inaki Tirados, Philippe Solano, Marina Antillon, Albert Picado, Severin Mbainda, Justin Darnas, Emily H Crowley, Steve J Torr, Mallaye Peka","doi":"10.1186/s40249-022-00934-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In recent years, a programme of vector control, screening and treatment of gambiense human African trypanosomiasis (gHAT) infections led to a rapid decline in cases in the Mandoul focus of Chad. To represent the biology of transmission between humans and tsetse, we previously developed a mechanistic transmission model, fitted to data between 2000 and 2013 which suggested that transmission was interrupted by 2015. The present study outlines refinements to the model to: (1) Assess whether elimination of transmission has already been achieved despite low-level case reporting; (2) quantify the role of intensified interventions in transmission reduction; and (3) predict the trajectory of gHAT in Mandoul for the next decade under different strategies.</p><p><strong>Method: </strong>Our previous gHAT transmission model for Mandoul was updated using human case data (2000-2019) and a series of model refinements. These include how diagnostic specificity is incorporated into the model and improvements to the fitting method (increased variance in observed case reporting and how underreporting and improvements to passive screening are captured). A side-by-side comparison of fitting to case data was performed between the models.</p><p><strong>Results: </strong>We estimated that passive detection rates have increased due to improvements in diagnostic availability in fixed health facilities since 2015, by 2.1-fold for stage 1 detection, and 1.5-fold for stage 2. We find that whilst the diagnostic algorithm for active screening is estimated to be highly specific (95% credible interval (CI) 99.9-100%, Specificity = 99.9%), the high screening and low infection levels mean that some recently reported cases with no parasitological confirmation might be false positives. We also find that the focus-wide tsetse reduction estimated through model fitting (95% CI 96.1-99.6%, Reduction = 99.1%) is comparable to the reduction previously measured by the decline in tsetse catches from monitoring traps. In line with previous results, the model suggests that transmission was interrupted in 2015 due to intensified interventions.</p><p><strong>Conclusions: </strong>We recommend that additional confirmatory testing is performed in Mandoul to ensure the endgame can be carefully monitored. More specific measurement of cases, would better inform when it is safe to stop active screening and vector control, provided there is a strong passive surveillance system in place.</p>","PeriodicalId":13587,"journal":{"name":"Infectious Diseases of Poverty","volume":"11 1","pages":"11"},"PeriodicalIF":5.5000,"publicationDate":"2022-01-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8785021/pdf/","citationCount":"0","resultStr":"{\"title\":\"Update of transmission modelling and projections of gambiense human African trypanosomiasis in the Mandoul focus, Chad.\",\"authors\":\"Kat S Rock, Ching-I Huang, Ronald E Crump, Paul R Bessell, Paul E Brown, Inaki Tirados, Philippe Solano, Marina Antillon, Albert Picado, Severin Mbainda, Justin Darnas, Emily H Crowley, Steve J Torr, Mallaye Peka\",\"doi\":\"10.1186/s40249-022-00934-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>In recent years, a programme of vector control, screening and treatment of gambiense human African trypanosomiasis (gHAT) infections led to a rapid decline in cases in the Mandoul focus of Chad. To represent the biology of transmission between humans and tsetse, we previously developed a mechanistic transmission model, fitted to data between 2000 and 2013 which suggested that transmission was interrupted by 2015. The present study outlines refinements to the model to: (1) Assess whether elimination of transmission has already been achieved despite low-level case reporting; (2) quantify the role of intensified interventions in transmission reduction; and (3) predict the trajectory of gHAT in Mandoul for the next decade under different strategies.</p><p><strong>Method: </strong>Our previous gHAT transmission model for Mandoul was updated using human case data (2000-2019) and a series of model refinements. These include how diagnostic specificity is incorporated into the model and improvements to the fitting method (increased variance in observed case reporting and how underreporting and improvements to passive screening are captured). A side-by-side comparison of fitting to case data was performed between the models.</p><p><strong>Results: </strong>We estimated that passive detection rates have increased due to improvements in diagnostic availability in fixed health facilities since 2015, by 2.1-fold for stage 1 detection, and 1.5-fold for stage 2. We find that whilst the diagnostic algorithm for active screening is estimated to be highly specific (95% credible interval (CI) 99.9-100%, Specificity = 99.9%), the high screening and low infection levels mean that some recently reported cases with no parasitological confirmation might be false positives. We also find that the focus-wide tsetse reduction estimated through model fitting (95% CI 96.1-99.6%, Reduction = 99.1%) is comparable to the reduction previously measured by the decline in tsetse catches from monitoring traps. In line with previous results, the model suggests that transmission was interrupted in 2015 due to intensified interventions.</p><p><strong>Conclusions: </strong>We recommend that additional confirmatory testing is performed in Mandoul to ensure the endgame can be carefully monitored. More specific measurement of cases, would better inform when it is safe to stop active screening and vector control, provided there is a strong passive surveillance system in place.</p>\",\"PeriodicalId\":13587,\"journal\":{\"name\":\"Infectious Diseases of Poverty\",\"volume\":\"11 1\",\"pages\":\"11\"},\"PeriodicalIF\":5.5000,\"publicationDate\":\"2022-01-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8785021/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Infectious Diseases of Poverty\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s40249-022-00934-8\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"INFECTIOUS DISEASES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious Diseases of Poverty","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40249-022-00934-8","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
Update of transmission modelling and projections of gambiense human African trypanosomiasis in the Mandoul focus, Chad.
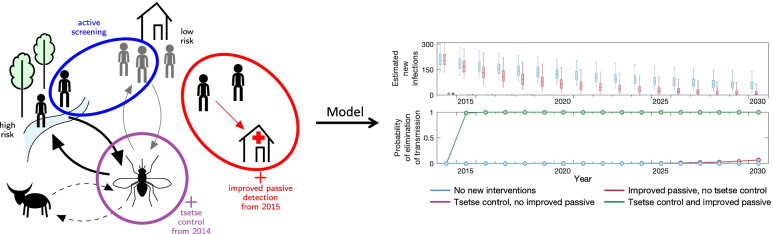
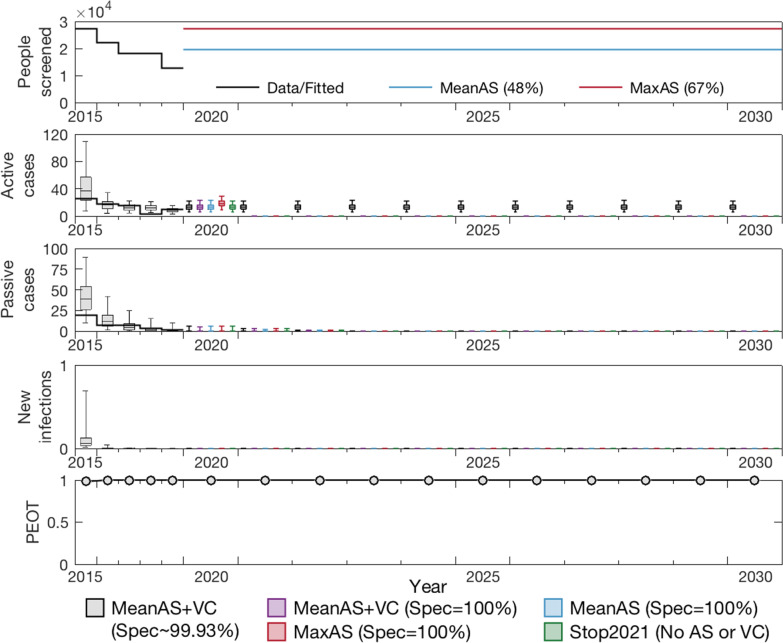
Background: In recent years, a programme of vector control, screening and treatment of gambiense human African trypanosomiasis (gHAT) infections led to a rapid decline in cases in the Mandoul focus of Chad. To represent the biology of transmission between humans and tsetse, we previously developed a mechanistic transmission model, fitted to data between 2000 and 2013 which suggested that transmission was interrupted by 2015. The present study outlines refinements to the model to: (1) Assess whether elimination of transmission has already been achieved despite low-level case reporting; (2) quantify the role of intensified interventions in transmission reduction; and (3) predict the trajectory of gHAT in Mandoul for the next decade under different strategies.
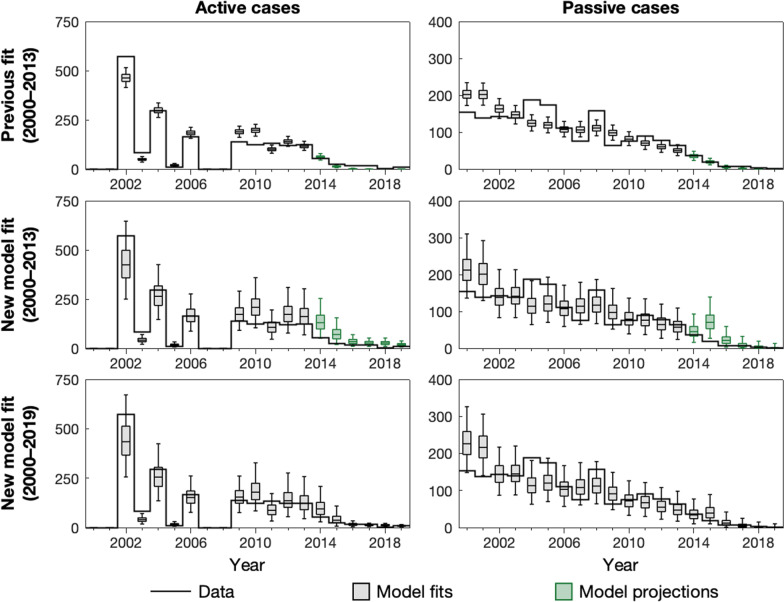
Method: Our previous gHAT transmission model for Mandoul was updated using human case data (2000-2019) and a series of model refinements. These include how diagnostic specificity is incorporated into the model and improvements to the fitting method (increased variance in observed case reporting and how underreporting and improvements to passive screening are captured). A side-by-side comparison of fitting to case data was performed between the models.
Results: We estimated that passive detection rates have increased due to improvements in diagnostic availability in fixed health facilities since 2015, by 2.1-fold for stage 1 detection, and 1.5-fold for stage 2. We find that whilst the diagnostic algorithm for active screening is estimated to be highly specific (95% credible interval (CI) 99.9-100%, Specificity = 99.9%), the high screening and low infection levels mean that some recently reported cases with no parasitological confirmation might be false positives. We also find that the focus-wide tsetse reduction estimated through model fitting (95% CI 96.1-99.6%, Reduction = 99.1%) is comparable to the reduction previously measured by the decline in tsetse catches from monitoring traps. In line with previous results, the model suggests that transmission was interrupted in 2015 due to intensified interventions.
Conclusions: We recommend that additional confirmatory testing is performed in Mandoul to ensure the endgame can be carefully monitored. More specific measurement of cases, would better inform when it is safe to stop active screening and vector control, provided there is a strong passive surveillance system in place.
期刊介绍:
Infectious Diseases of Poverty is a peer-reviewed, open access journal that focuses on essential public health questions related to infectious diseases of poverty. It covers a wide range of topics and methods, including the biology of pathogens and vectors, diagnosis and detection, treatment and case management, epidemiology and modeling, zoonotic hosts and animal reservoirs, control strategies and implementation, new technologies, and their application.
The journal also explores the impact of transdisciplinary or multisectoral approaches on health systems, ecohealth, environmental management, and innovative technologies. It aims to provide a platform for the exchange of research and ideas that can contribute to the improvement of public health in resource-limited settings.
In summary, Infectious Diseases of Poverty aims to address the urgent challenges posed by infectious diseases in impoverished populations. By publishing high-quality research in various areas, the journal seeks to advance our understanding of these diseases and contribute to the development of effective strategies for prevention, diagnosis, and treatment.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


