Rachel C Sisodia, Dan Ellis, Michael Hidrue, Pamela Linov, Elena Cavallo, Allison S Bryant, May Wakamatsu, Marcela G Del Carmen
{"title":"个体术后增强康复方案组成对住院时间影响的队列研究。","authors":"Rachel C Sisodia, Dan Ellis, Michael Hidrue, Pamela Linov, Elena Cavallo, Allison S Bryant, May Wakamatsu, Marcela G Del Carmen","doi":"10.1136/bmjsit-2021-000087","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The goal of this study was to explore which enhanced recovery after surgery (ERAS) bundle items were most associated with decreased length of stay after surgery, most likely associated with decreased length of stay after surgery.</p><p><strong>Design: </strong>A cohort study.</p><p><strong>Setting: </strong>Large tertiary academic medical centre.</p><p><strong>Participants: </strong>The study included 1318 women undergoing hysterectomy as part of our ERAS pathway between 1 February 2018 and 30 January 2020 and a matched historical cohort of all hysterectomies performed at our institution between 3 October 2016 and 30 January 2018 (n=1063).</p><p><strong>Intervention: </strong>The addition of ERAS to perioperative care.This is a cohort study of all patients undergoing hysterectomy at an academic medical centre after ERAS implementation on 1 February 2018. Compliance and outcomes after ERAS roll out were monitored and managed by a centralised team. Descriptive statistics, multivariate regression, interrupted time series analysis were used as indicated.</p><p><strong>Main outcome measures: </strong>Impact of ERAS process measure adherence on length of stay.</p><p><strong>Results: </strong>After initiation of ERAS pathway, 1318 women underwent hysterectomy. There were more open surgeries after ERAS implementation, but cohorts were otherwise balanced. The impact of process measure adherence on length of stay varied based on surgical approach (minimally invasive vs open). For open surgery, compliance with intraoperative antiemetics (-30%, 95% CI -18% to 40%) and decreased postoperative fluid administration (-12%, 95% CI -1% to 21%) were significantly associated with reduced length of stay. For minimally invasive surgery, ambulation within 8 hours of surgery was associated with reduced length of stay (-53%, 95% CI -55% to 52%).</p><p><strong>Conclusions: </strong>While adherence to overall ERAS protocols decreases length of stay, the specific components of the bundle most significantly impacting this outcome remain elusive. Our data identify early ambulation, use of antiemetics and decreasing postoperative fluid administration to be associated with decreased length of stay.</p>","PeriodicalId":33349,"journal":{"name":"BMJ Surgery Interventions Health Technologies","volume":"3 1","pages":"e000087"},"PeriodicalIF":2.1000,"publicationDate":"2021-09-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/52/4b/bmjsit-2021-000087.PMC8749327.pdf","citationCount":"0","resultStr":"{\"title\":\"Cohort study of impact on length of stay of individual enhanced recovery after surgery protocol components.\",\"authors\":\"Rachel C Sisodia, Dan Ellis, Michael Hidrue, Pamela Linov, Elena Cavallo, Allison S Bryant, May Wakamatsu, Marcela G Del Carmen\",\"doi\":\"10.1136/bmjsit-2021-000087\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>The goal of this study was to explore which enhanced recovery after surgery (ERAS) bundle items were most associated with decreased length of stay after surgery, most likely associated with decreased length of stay after surgery.</p><p><strong>Design: </strong>A cohort study.</p><p><strong>Setting: </strong>Large tertiary academic medical centre.</p><p><strong>Participants: </strong>The study included 1318 women undergoing hysterectomy as part of our ERAS pathway between 1 February 2018 and 30 January 2020 and a matched historical cohort of all hysterectomies performed at our institution between 3 October 2016 and 30 January 2018 (n=1063).</p><p><strong>Intervention: </strong>The addition of ERAS to perioperative care.This is a cohort study of all patients undergoing hysterectomy at an academic medical centre after ERAS implementation on 1 February 2018. Compliance and outcomes after ERAS roll out were monitored and managed by a centralised team. Descriptive statistics, multivariate regression, interrupted time series analysis were used as indicated.</p><p><strong>Main outcome measures: </strong>Impact of ERAS process measure adherence on length of stay.</p><p><strong>Results: </strong>After initiation of ERAS pathway, 1318 women underwent hysterectomy. There were more open surgeries after ERAS implementation, but cohorts were otherwise balanced. The impact of process measure adherence on length of stay varied based on surgical approach (minimally invasive vs open). For open surgery, compliance with intraoperative antiemetics (-30%, 95% CI -18% to 40%) and decreased postoperative fluid administration (-12%, 95% CI -1% to 21%) were significantly associated with reduced length of stay. For minimally invasive surgery, ambulation within 8 hours of surgery was associated with reduced length of stay (-53%, 95% CI -55% to 52%).</p><p><strong>Conclusions: </strong>While adherence to overall ERAS protocols decreases length of stay, the specific components of the bundle most significantly impacting this outcome remain elusive. Our data identify early ambulation, use of antiemetics and decreasing postoperative fluid administration to be associated with decreased length of stay.</p>\",\"PeriodicalId\":33349,\"journal\":{\"name\":\"BMJ Surgery Interventions Health Technologies\",\"volume\":\"3 1\",\"pages\":\"e000087\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2021-09-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/52/4b/bmjsit-2021-000087.PMC8749327.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Surgery Interventions Health Technologies\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjsit-2021-000087\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Surgery Interventions Health Technologies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjsit-2021-000087","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
摘要
目的:本研究的目的是探讨哪些增强术后恢复(ERAS)捆绑项目与术后住院时间缩短最相关,最有可能与术后住院时间缩短相关。设计:队列研究。环境:大型三级学术医疗中心。参与者:该研究包括2018年2月1日至2020年1月30日期间接受子宫切除术的1318名女性,以及2016年10月3日至2018年1月30日期间在我们机构进行的所有子宫切除术的匹配历史队列(n=1063)。干预措施:在围手术期护理中加入ERAS。这是一项队列研究,研究对象是2018年2月1日实施ERAS后在学术医疗中心接受子宫切除术的所有患者。ERAS推出后的合规性和结果由集中团队监控和管理。采用描述性统计、多元回归、中断时间序列分析。主要结果测量:ERAS过程测量依从性对住院时间的影响。结果:经ERAS通路启动后,1318例妇女行子宫切除术。ERAS实施后开放性手术较多,但队列是平衡的。过程测量依从性对住院时间的影响因手术入路(微创与开放)而异。对于开放手术,术中止吐药的依从性(-30%,95% CI -18%至40%)和术后液体给药的减少(-12%,95% CI -1%至21%)与住院时间的缩短显著相关。对于微创手术,手术8小时内走动与住院时间缩短相关(-53%,95% CI -55%至52%)。结论:虽然总体ERAS方案的依从性减少了住院时间,但对该结果影响最大的具体组成部分仍然难以捉摸。我们的数据表明,早期下床、使用止吐药和减少术后液体给药与住院时间缩短有关。
Cohort study of impact on length of stay of individual enhanced recovery after surgery protocol components.
Objective: The goal of this study was to explore which enhanced recovery after surgery (ERAS) bundle items were most associated with decreased length of stay after surgery, most likely associated with decreased length of stay after surgery.
Design: A cohort study.
Setting: Large tertiary academic medical centre.
Participants: The study included 1318 women undergoing hysterectomy as part of our ERAS pathway between 1 February 2018 and 30 January 2020 and a matched historical cohort of all hysterectomies performed at our institution between 3 October 2016 and 30 January 2018 (n=1063).
Intervention: The addition of ERAS to perioperative care.This is a cohort study of all patients undergoing hysterectomy at an academic medical centre after ERAS implementation on 1 February 2018. Compliance and outcomes after ERAS roll out were monitored and managed by a centralised team. Descriptive statistics, multivariate regression, interrupted time series analysis were used as indicated.
Main outcome measures: Impact of ERAS process measure adherence on length of stay.
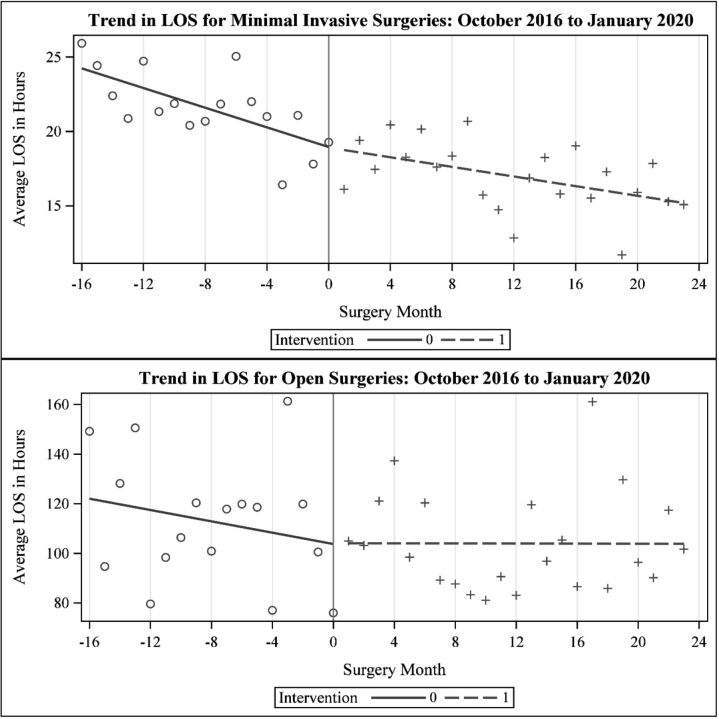
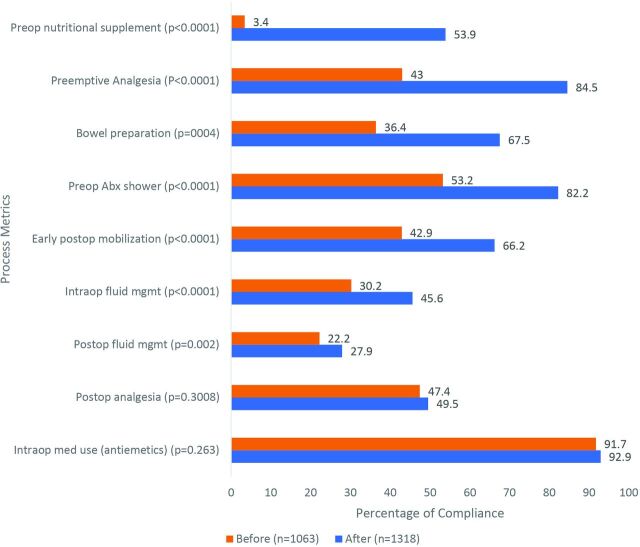
Results: After initiation of ERAS pathway, 1318 women underwent hysterectomy. There were more open surgeries after ERAS implementation, but cohorts were otherwise balanced. The impact of process measure adherence on length of stay varied based on surgical approach (minimally invasive vs open). For open surgery, compliance with intraoperative antiemetics (-30%, 95% CI -18% to 40%) and decreased postoperative fluid administration (-12%, 95% CI -1% to 21%) were significantly associated with reduced length of stay. For minimally invasive surgery, ambulation within 8 hours of surgery was associated with reduced length of stay (-53%, 95% CI -55% to 52%).
Conclusions: While adherence to overall ERAS protocols decreases length of stay, the specific components of the bundle most significantly impacting this outcome remain elusive. Our data identify early ambulation, use of antiemetics and decreasing postoperative fluid administration to be associated with decreased length of stay.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


