Lourens Jan Peter Nonkes, Valérie de Haas, Hans Kemperman, Albert Huisman, Ruben Eduardus Antonius Musson, Wouter Marcel Tiel Groenestege
{"title":"评估和处理白血病患儿白血病溶解介导的假性高钾血症。","authors":"Lourens Jan Peter Nonkes, Valérie de Haas, Hans Kemperman, Albert Huisman, Ruben Eduardus Antonius Musson, Wouter Marcel Tiel Groenestege","doi":"10.11613/BM.2022.010904","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Leukolysis-related pseudohyperkalemia due to preanalytical procedures may lead to erroneous (or absence of) treatment based on an invalid lab test result. We aimed to obtain a leukocyte threshold above which leukolysis-related pseudohyperkalemia becomes clinical relevant. Secondly, temporal dynamics of treatment-induced leukocyte decrease were studied to allow tailored implementation of laboratory information system (LIS) decision rules based on the leukocyte threshold to avoid leukolysis-related pseudohyperkalemia.</p><p><strong>Materials and methods: </strong>Potassium results of AU5811 routine chemistry (Beckman Coulter, Brea, California, USA) and iStat point of care (POC) (Abbott Diagnostics, Chicago, Illinois, USA) analysers were compared, the latter method being insensitive to leukolysis caused by pre-analytical procedures. Potassium results were combined with leukocyte counts obtained using a Cell-Dyn Sapphire haematology analyser (Abbott Diagnostics, Santa Clara, California, USA), resulting in 132 unique data triplets. Regression analysis was performed to establish a leukocyte threshold. The Reference Change Value (√2 x Z x √(CV<sub>a</sub> <sup>2</sup> + CV<sub>i</sub> <sup>2</sup>)) was used to calculate maximum allowable difference between routine analyser and POC potassium results (delta<sub>max</sub> + 0.58 mmol/L). Temporal analysis on the treatment-induced leukocyte decrease was performed by plotting leukocyte counts in time for all patients above the threshold leukocyte count (N = 41).</p><p><strong>Results: </strong>Established leukocyte threshold was 63 x10<sup>9</sup>/L. Temporal analysis showed leukocyte counts below the threshold within 8 days of treatment for all patients.</p><p><strong>Conclusions: </strong>Based on performed analyses we were able to implement LIS decision rules to reduce pseudohyperkalemia due to preanalytical procedures. This implementation can contribute to a reduction in erroneous (or absence of) treatments in the clinic.</p>","PeriodicalId":9021,"journal":{"name":"Biochemia Medica","volume":"32 1","pages":"010904"},"PeriodicalIF":1.8000,"publicationDate":"2022-02-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8833246/pdf/","citationCount":"1","resultStr":"{\"title\":\"Evaluation and management of leukolysis-mediated pseudohyperkalemia in paediatric leukemic samples.\",\"authors\":\"Lourens Jan Peter Nonkes, Valérie de Haas, Hans Kemperman, Albert Huisman, Ruben Eduardus Antonius Musson, Wouter Marcel Tiel Groenestege\",\"doi\":\"10.11613/BM.2022.010904\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Leukolysis-related pseudohyperkalemia due to preanalytical procedures may lead to erroneous (or absence of) treatment based on an invalid lab test result. We aimed to obtain a leukocyte threshold above which leukolysis-related pseudohyperkalemia becomes clinical relevant. Secondly, temporal dynamics of treatment-induced leukocyte decrease were studied to allow tailored implementation of laboratory information system (LIS) decision rules based on the leukocyte threshold to avoid leukolysis-related pseudohyperkalemia.</p><p><strong>Materials and methods: </strong>Potassium results of AU5811 routine chemistry (Beckman Coulter, Brea, California, USA) and iStat point of care (POC) (Abbott Diagnostics, Chicago, Illinois, USA) analysers were compared, the latter method being insensitive to leukolysis caused by pre-analytical procedures. Potassium results were combined with leukocyte counts obtained using a Cell-Dyn Sapphire haematology analyser (Abbott Diagnostics, Santa Clara, California, USA), resulting in 132 unique data triplets. Regression analysis was performed to establish a leukocyte threshold. The Reference Change Value (√2 x Z x √(CV<sub>a</sub> <sup>2</sup> + CV<sub>i</sub> <sup>2</sup>)) was used to calculate maximum allowable difference between routine analyser and POC potassium results (delta<sub>max</sub> + 0.58 mmol/L). Temporal analysis on the treatment-induced leukocyte decrease was performed by plotting leukocyte counts in time for all patients above the threshold leukocyte count (N = 41).</p><p><strong>Results: </strong>Established leukocyte threshold was 63 x10<sup>9</sup>/L. Temporal analysis showed leukocyte counts below the threshold within 8 days of treatment for all patients.</p><p><strong>Conclusions: </strong>Based on performed analyses we were able to implement LIS decision rules to reduce pseudohyperkalemia due to preanalytical procedures. This implementation can contribute to a reduction in erroneous (or absence of) treatments in the clinic.</p>\",\"PeriodicalId\":9021,\"journal\":{\"name\":\"Biochemia Medica\",\"volume\":\"32 1\",\"pages\":\"010904\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2022-02-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8833246/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Biochemia Medica\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.11613/BM.2022.010904\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICAL LABORATORY TECHNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Biochemia Medica","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.11613/BM.2022.010904","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICAL LABORATORY TECHNOLOGY","Score":null,"Total":0}
Evaluation and management of leukolysis-mediated pseudohyperkalemia in paediatric leukemic samples.
Introduction: Leukolysis-related pseudohyperkalemia due to preanalytical procedures may lead to erroneous (or absence of) treatment based on an invalid lab test result. We aimed to obtain a leukocyte threshold above which leukolysis-related pseudohyperkalemia becomes clinical relevant. Secondly, temporal dynamics of treatment-induced leukocyte decrease were studied to allow tailored implementation of laboratory information system (LIS) decision rules based on the leukocyte threshold to avoid leukolysis-related pseudohyperkalemia.
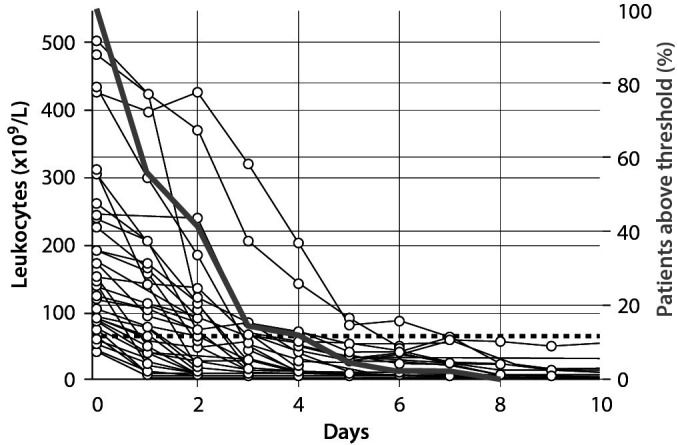
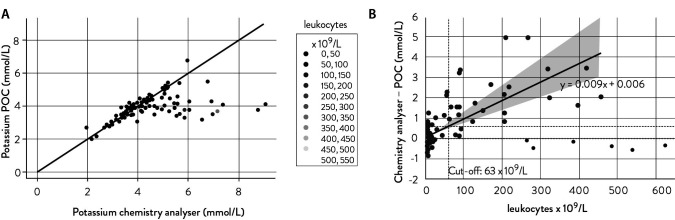
Materials and methods: Potassium results of AU5811 routine chemistry (Beckman Coulter, Brea, California, USA) and iStat point of care (POC) (Abbott Diagnostics, Chicago, Illinois, USA) analysers were compared, the latter method being insensitive to leukolysis caused by pre-analytical procedures. Potassium results were combined with leukocyte counts obtained using a Cell-Dyn Sapphire haematology analyser (Abbott Diagnostics, Santa Clara, California, USA), resulting in 132 unique data triplets. Regression analysis was performed to establish a leukocyte threshold. The Reference Change Value (√2 x Z x √(CVa2 + CVi2)) was used to calculate maximum allowable difference between routine analyser and POC potassium results (deltamax + 0.58 mmol/L). Temporal analysis on the treatment-induced leukocyte decrease was performed by plotting leukocyte counts in time for all patients above the threshold leukocyte count (N = 41).
Results: Established leukocyte threshold was 63 x109/L. Temporal analysis showed leukocyte counts below the threshold within 8 days of treatment for all patients.
Conclusions: Based on performed analyses we were able to implement LIS decision rules to reduce pseudohyperkalemia due to preanalytical procedures. This implementation can contribute to a reduction in erroneous (or absence of) treatments in the clinic.
期刊介绍:
Biochemia Medica is the official peer-reviewed journal of the Croatian Society of Medical Biochemistry and Laboratory Medicine. Journal provides a wide coverage of research in all aspects of clinical chemistry and laboratory medicine. Following categories fit into the scope of the Journal: general clinical chemistry, haematology and haemostasis, molecular diagnostics and endocrinology. Development, validation and verification of analytical techniques and methods applicable to clinical chemistry and laboratory medicine are welcome as well as studies dealing with laboratory organization, automation and quality control. Journal publishes on a regular basis educative preanalytical case reports (Preanalytical mysteries), articles dealing with applied biostatistics (Lessons in biostatistics) and research integrity (Research integrity corner).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


