SungJoon Park, Sung Woo Lee, Kap Su Han, Eui Jung Lee, Dong-Hyun Jang, Si Jin Lee, Ji Sung Lee, Su Jin Kim
{"title":"院外心脏骤停后对神经系统预后有利的最佳心肺复苏时间。","authors":"SungJoon Park, Sung Woo Lee, Kap Su Han, Eui Jung Lee, Dong-Hyun Jang, Si Jin Lee, Ji Sung Lee, Su Jin Kim","doi":"10.1186/s13049-022-00993-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A favorable neurological outcome is closely related to patient characteristics and total cardiopulmonary resuscitation (CPR) duration. The total CPR duration consists of pre-hospital and in-hospital durations. To date, consensus is lacking on the optimal total CPR duration. Therefore, this study aimed to determine the upper limit of total CPR duration, the optimal cut-off time at the pre-hospital level, and the time to switch from conventional CPR to alternative CPR such as extracorporeal CPR.</p><p><strong>Methods: </strong>We conducted a retrospective observational study using prospective, multi-center registry of out-of-hospital cardiac arrest (OHCA) patients between October 2015 and June 2019. Emergency medical service-assessed adult patients (aged ≥ 18 years) with non-traumatic OHCA were included. The primary endpoint was a favorable neurological outcome at hospital discharge.</p><p><strong>Results: </strong>Among 7914 patients with OHCA, 577 had favorable neurological outcomes. The optimal cut-off for pre-hospital CPR duration in patients with OHCA was 12 min regardless of the initial rhythm. The optimal cut-offs for total CPR duration that transitioned from conventional CPR to an alternative CPR method were 25 and 21 min in patients with initial shockable and non-shockable rhythms, respectively. In the two groups, the upper limits of total CPR duration for achieving a probability of favorable neurological outcomes < 1% were 55-62 and 24-34 min, respectively, while those for a cumulative proportion of favorable neurological outcome > 99% were 43-53 and 45-71 min, respectively.</p><p><strong>Conclusions: </strong>Herein, we identified the optimal cut-off time for transitioning from pre-hospital to in-hospital settings and from conventional CPR to alternative resuscitation. Although there is an upper limit of CPR duration, favorable neurological outcomes can be expected according to each patient's resuscitation-related factors, despite prolonged CPR duration.</p>","PeriodicalId":501057,"journal":{"name":"Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine","volume":" ","pages":"5"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8760684/pdf/","citationCount":"10","resultStr":"{\"title\":\"Optimal cardiopulmonary resuscitation duration for favorable neurological outcomes after out-of-hospital cardiac arrest.\",\"authors\":\"SungJoon Park, Sung Woo Lee, Kap Su Han, Eui Jung Lee, Dong-Hyun Jang, Si Jin Lee, Ji Sung Lee, Su Jin Kim\",\"doi\":\"10.1186/s13049-022-00993-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>A favorable neurological outcome is closely related to patient characteristics and total cardiopulmonary resuscitation (CPR) duration. The total CPR duration consists of pre-hospital and in-hospital durations. To date, consensus is lacking on the optimal total CPR duration. Therefore, this study aimed to determine the upper limit of total CPR duration, the optimal cut-off time at the pre-hospital level, and the time to switch from conventional CPR to alternative CPR such as extracorporeal CPR.</p><p><strong>Methods: </strong>We conducted a retrospective observational study using prospective, multi-center registry of out-of-hospital cardiac arrest (OHCA) patients between October 2015 and June 2019. Emergency medical service-assessed adult patients (aged ≥ 18 years) with non-traumatic OHCA were included. The primary endpoint was a favorable neurological outcome at hospital discharge.</p><p><strong>Results: </strong>Among 7914 patients with OHCA, 577 had favorable neurological outcomes. The optimal cut-off for pre-hospital CPR duration in patients with OHCA was 12 min regardless of the initial rhythm. The optimal cut-offs for total CPR duration that transitioned from conventional CPR to an alternative CPR method were 25 and 21 min in patients with initial shockable and non-shockable rhythms, respectively. In the two groups, the upper limits of total CPR duration for achieving a probability of favorable neurological outcomes < 1% were 55-62 and 24-34 min, respectively, while those for a cumulative proportion of favorable neurological outcome > 99% were 43-53 and 45-71 min, respectively.</p><p><strong>Conclusions: </strong>Herein, we identified the optimal cut-off time for transitioning from pre-hospital to in-hospital settings and from conventional CPR to alternative resuscitation. Although there is an upper limit of CPR duration, favorable neurological outcomes can be expected according to each patient's resuscitation-related factors, despite prolonged CPR duration.</p>\",\"PeriodicalId\":501057,\"journal\":{\"name\":\"Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine\",\"volume\":\" \",\"pages\":\"5\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-01-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8760684/pdf/\",\"citationCount\":\"10\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13049-022-00993-8\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13049-022-00993-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Optimal cardiopulmonary resuscitation duration for favorable neurological outcomes after out-of-hospital cardiac arrest.
Background: A favorable neurological outcome is closely related to patient characteristics and total cardiopulmonary resuscitation (CPR) duration. The total CPR duration consists of pre-hospital and in-hospital durations. To date, consensus is lacking on the optimal total CPR duration. Therefore, this study aimed to determine the upper limit of total CPR duration, the optimal cut-off time at the pre-hospital level, and the time to switch from conventional CPR to alternative CPR such as extracorporeal CPR.
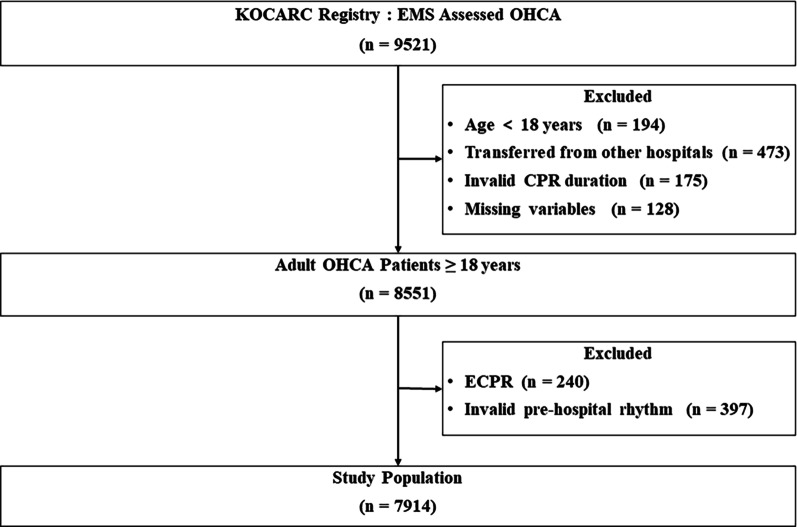
Methods: We conducted a retrospective observational study using prospective, multi-center registry of out-of-hospital cardiac arrest (OHCA) patients between October 2015 and June 2019. Emergency medical service-assessed adult patients (aged ≥ 18 years) with non-traumatic OHCA were included. The primary endpoint was a favorable neurological outcome at hospital discharge.
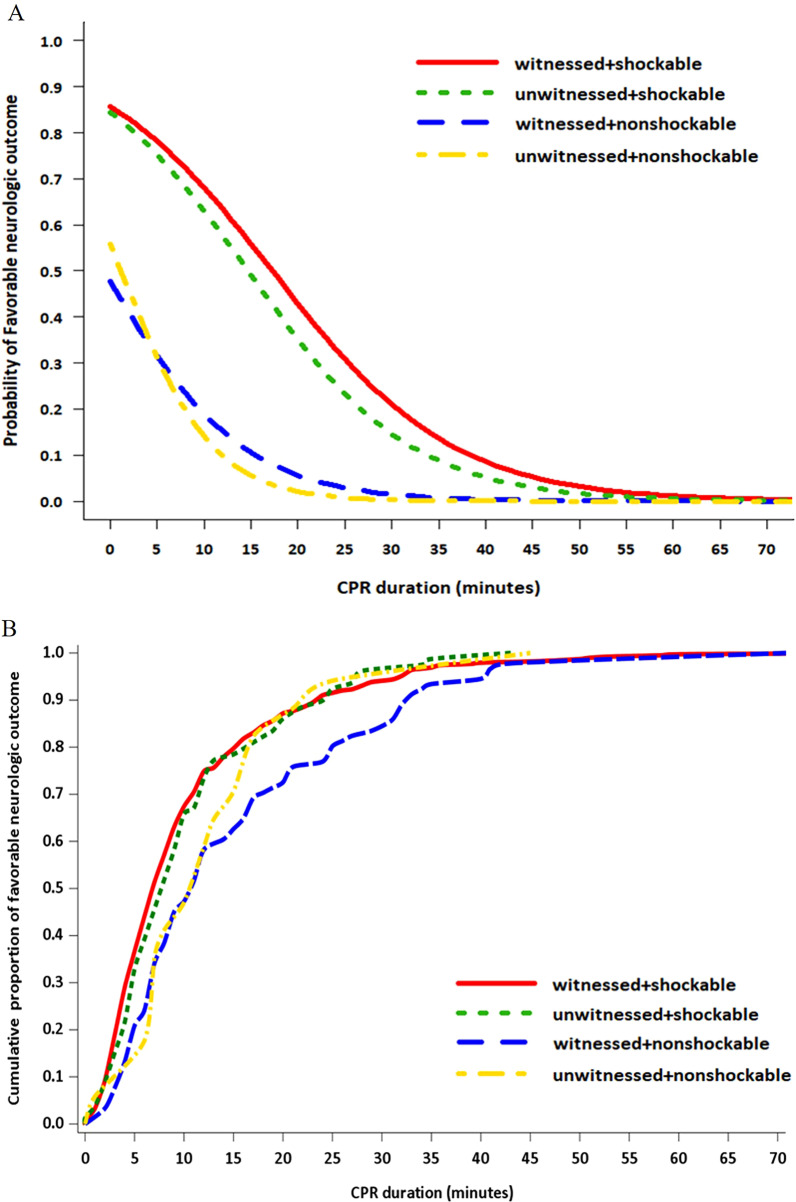
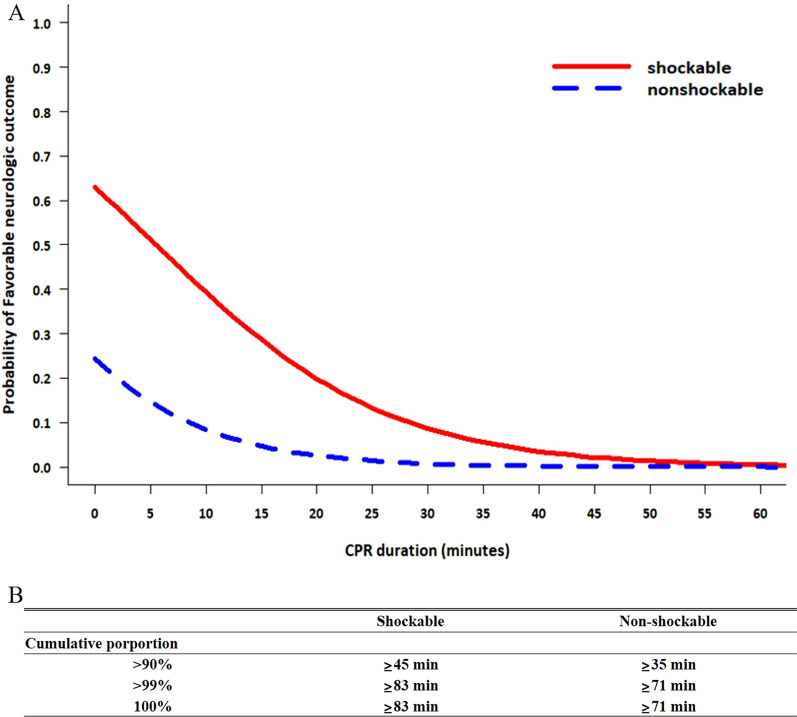
Results: Among 7914 patients with OHCA, 577 had favorable neurological outcomes. The optimal cut-off for pre-hospital CPR duration in patients with OHCA was 12 min regardless of the initial rhythm. The optimal cut-offs for total CPR duration that transitioned from conventional CPR to an alternative CPR method were 25 and 21 min in patients with initial shockable and non-shockable rhythms, respectively. In the two groups, the upper limits of total CPR duration for achieving a probability of favorable neurological outcomes < 1% were 55-62 and 24-34 min, respectively, while those for a cumulative proportion of favorable neurological outcome > 99% were 43-53 and 45-71 min, respectively.
Conclusions: Herein, we identified the optimal cut-off time for transitioning from pre-hospital to in-hospital settings and from conventional CPR to alternative resuscitation. Although there is an upper limit of CPR duration, favorable neurological outcomes can be expected according to each patient's resuscitation-related factors, despite prolonged CPR duration.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


