Ran Schwarzkopf, Morteza Meftah, Scott E Marwin, Michelle A Zabat, Jeffrey M Muir, Iain R Lamb
{"title":"应用无图像导航量化全膝关节置换术中的切割误差。","authors":"Ran Schwarzkopf, Morteza Meftah, Scott E Marwin, Michelle A Zabat, Jeffrey M Muir, Iain R Lamb","doi":"10.1186/s43019-021-00125-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Navigated total knee arthroplasty (TKA) improves implant alignment by providing feedback on resection parameters based on femoral and tibial cutting guide positions. However, saw blade thickness, deflection, and cutting guide motion may lead to final bone cuts differing from planned resections, potentially contributing to suboptimal component alignment. We used an imageless navigation device to intraoperatively quantify the magnitude of error between planned and actual resections, hypothesizing final bone cuts will differ from planned alignment.</p><p><strong>Materials and methods: </strong>A retrospective study including 60 consecutive patients undergoing primary TKA using a novel imageless navigation device was conducted. Device measurements of resection parameters were obtained via attachment of optical trackers to femoral and tibial cutting guides prior to resection. Following resection, optical trackers were placed directly on the bone cut surface and measurements were recorded. Cutting guide and bone resection measurements of both femoral and tibial varus/valgus, femoral flexion, tibial slope angles, and both femoral and tibial medial and lateral resection depths were compared using a Student's t-test.</p><p><strong>Results: </strong>Femoral cutting guide position differed from the actual cut by an average 0.6 ± 0.5° (p = 0.85) in the varus/valgus angle and 1.0 ± 1.0° (p = 0.003) in the flexion/extension angle. The difference between planned and actual cut measurements for medial and lateral femoral resection depth was 1.1 ± 1.1 mm (p = 0.32) and 1.2 ± 1.0 mm (p = 0.067), respectively. Planned cut measurements based on tibial guide position differed from the actual cut by an average of 0.9 ± 0.8° (p = 0.63) in the varus/valgus angle and 1.1 ± 1.0° (p = 0.95) in slope angle. Measurement of medial and lateral tibial resection depth differed by an average of 0.1 ± 1.8 mm (p = 0.78) and 0.2 ± 2.1 mm (p = 0.85), respectively.</p><p><strong>Conclusions: </strong>Significant discrepancies between planned and actual femoral bone resection were demonstrated for flexion/extension angle, likely the result of cutting error. Our data highlights the importance of cut verification postresection to confirm planned resections are achieved, and suggests imageless navigation may be a source of feedback that would allow surgeons to intraoperatively adjust resections to achieve optimal implant alignment.</p>","PeriodicalId":17886,"journal":{"name":"Knee Surgery & Related Research","volume":"33 1","pages":"43"},"PeriodicalIF":4.4000,"publicationDate":"2021-12-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8645113/pdf/","citationCount":"8","resultStr":"{\"title\":\"The use of imageless navigation to quantify cutting error in total knee arthroplasty.\",\"authors\":\"Ran Schwarzkopf, Morteza Meftah, Scott E Marwin, Michelle A Zabat, Jeffrey M Muir, Iain R Lamb\",\"doi\":\"10.1186/s43019-021-00125-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Navigated total knee arthroplasty (TKA) improves implant alignment by providing feedback on resection parameters based on femoral and tibial cutting guide positions. However, saw blade thickness, deflection, and cutting guide motion may lead to final bone cuts differing from planned resections, potentially contributing to suboptimal component alignment. We used an imageless navigation device to intraoperatively quantify the magnitude of error between planned and actual resections, hypothesizing final bone cuts will differ from planned alignment.</p><p><strong>Materials and methods: </strong>A retrospective study including 60 consecutive patients undergoing primary TKA using a novel imageless navigation device was conducted. Device measurements of resection parameters were obtained via attachment of optical trackers to femoral and tibial cutting guides prior to resection. Following resection, optical trackers were placed directly on the bone cut surface and measurements were recorded. Cutting guide and bone resection measurements of both femoral and tibial varus/valgus, femoral flexion, tibial slope angles, and both femoral and tibial medial and lateral resection depths were compared using a Student's t-test.</p><p><strong>Results: </strong>Femoral cutting guide position differed from the actual cut by an average 0.6 ± 0.5° (p = 0.85) in the varus/valgus angle and 1.0 ± 1.0° (p = 0.003) in the flexion/extension angle. The difference between planned and actual cut measurements for medial and lateral femoral resection depth was 1.1 ± 1.1 mm (p = 0.32) and 1.2 ± 1.0 mm (p = 0.067), respectively. Planned cut measurements based on tibial guide position differed from the actual cut by an average of 0.9 ± 0.8° (p = 0.63) in the varus/valgus angle and 1.1 ± 1.0° (p = 0.95) in slope angle. Measurement of medial and lateral tibial resection depth differed by an average of 0.1 ± 1.8 mm (p = 0.78) and 0.2 ± 2.1 mm (p = 0.85), respectively.</p><p><strong>Conclusions: </strong>Significant discrepancies between planned and actual femoral bone resection were demonstrated for flexion/extension angle, likely the result of cutting error. Our data highlights the importance of cut verification postresection to confirm planned resections are achieved, and suggests imageless navigation may be a source of feedback that would allow surgeons to intraoperatively adjust resections to achieve optimal implant alignment.</p>\",\"PeriodicalId\":17886,\"journal\":{\"name\":\"Knee Surgery & Related Research\",\"volume\":\"33 1\",\"pages\":\"43\"},\"PeriodicalIF\":4.4000,\"publicationDate\":\"2021-12-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8645113/pdf/\",\"citationCount\":\"8\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Knee Surgery & Related Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s43019-021-00125-z\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Knee Surgery & Related Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s43019-021-00125-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 8
摘要
目的:导航全膝关节置换术(TKA)通过提供基于股骨和胫骨切割导向位置的切除参数反馈来改善假体对齐。然而,锯片厚度、挠度和切割导轨运动可能导致最终的骨切割与计划切除不同,可能导致部件对准不理想。我们使用无图像导航装置术中量化计划和实际切除之间的误差大小,假设最终的骨切割将不同于计划的对齐。材料和方法:回顾性研究包括60例使用新型无图像导航装置进行原发性TKA的患者。在切除前,通过将光学跟踪器附着在股骨和胫骨切割导轨上获得切除参数的设备测量。切除后,将光学跟踪器直接放置在骨切割表面并记录测量结果。采用Student's t检验比较股骨和胫骨内翻/外翻、股骨屈曲、胫骨斜角以及股骨和胫骨内侧和外侧切除深度的切割导轨和骨切除测量值。结果:股骨内翻角与实际切割位置平均相差0.6±0.5°(p = 0.85),屈伸角与实际切割位置平均相差1.0±1.0°(p = 0.003)。股骨内侧和外侧切除深度的计划与实际切割测量值的差异分别为1.1±1.1 mm (p = 0.32)和1.2±1.0 mm (p = 0.067)。基于胫骨导向位置的计划切口测量值与实际切口在内翻/外翻角上平均相差0.9±0.8°(p = 0.63),在斜角上平均相差1.1±1.0°(p = 0.95)。测量胫骨内侧和外侧切除深度的平均差异分别为0.1±1.8 mm (p = 0.78)和0.2±2.1 mm (p = 0.85)。结论:计划和实际股骨切除在屈伸角度上存在显著差异,这可能是切割错误的结果。我们的数据强调了切除后切口验证的重要性,以确认计划切除的实现,并建议无图像导航可能是一种反馈来源,允许外科医生术中调整切除以达到最佳种植体对齐。
The use of imageless navigation to quantify cutting error in total knee arthroplasty.
Purpose: Navigated total knee arthroplasty (TKA) improves implant alignment by providing feedback on resection parameters based on femoral and tibial cutting guide positions. However, saw blade thickness, deflection, and cutting guide motion may lead to final bone cuts differing from planned resections, potentially contributing to suboptimal component alignment. We used an imageless navigation device to intraoperatively quantify the magnitude of error between planned and actual resections, hypothesizing final bone cuts will differ from planned alignment.
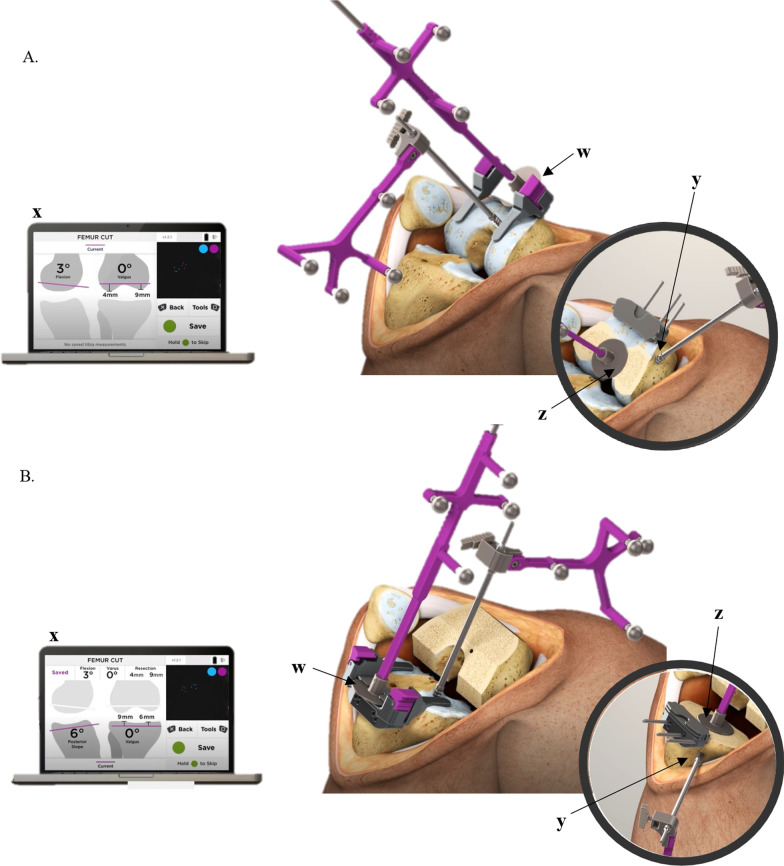
Materials and methods: A retrospective study including 60 consecutive patients undergoing primary TKA using a novel imageless navigation device was conducted. Device measurements of resection parameters were obtained via attachment of optical trackers to femoral and tibial cutting guides prior to resection. Following resection, optical trackers were placed directly on the bone cut surface and measurements were recorded. Cutting guide and bone resection measurements of both femoral and tibial varus/valgus, femoral flexion, tibial slope angles, and both femoral and tibial medial and lateral resection depths were compared using a Student's t-test.
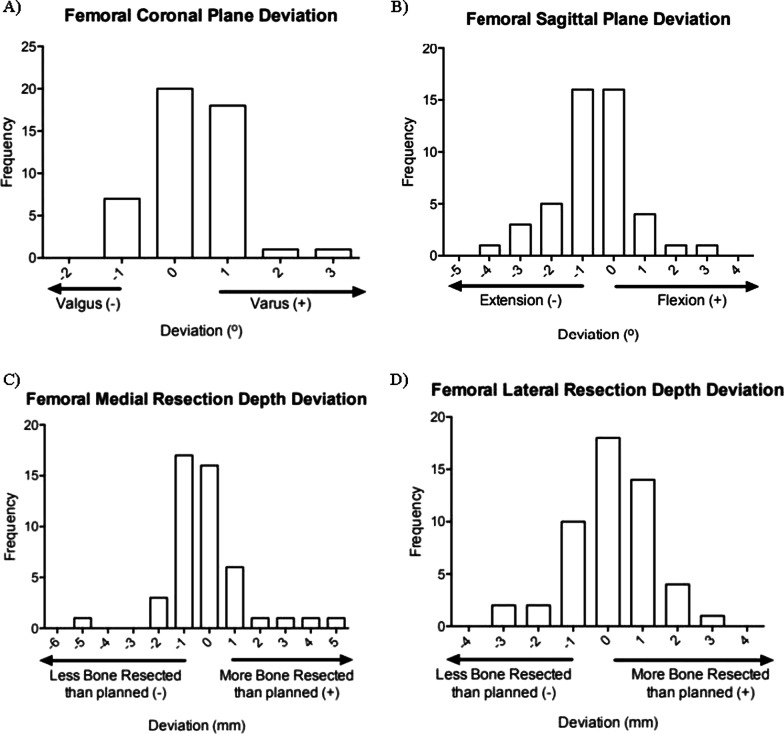
Results: Femoral cutting guide position differed from the actual cut by an average 0.6 ± 0.5° (p = 0.85) in the varus/valgus angle and 1.0 ± 1.0° (p = 0.003) in the flexion/extension angle. The difference between planned and actual cut measurements for medial and lateral femoral resection depth was 1.1 ± 1.1 mm (p = 0.32) and 1.2 ± 1.0 mm (p = 0.067), respectively. Planned cut measurements based on tibial guide position differed from the actual cut by an average of 0.9 ± 0.8° (p = 0.63) in the varus/valgus angle and 1.1 ± 1.0° (p = 0.95) in slope angle. Measurement of medial and lateral tibial resection depth differed by an average of 0.1 ± 1.8 mm (p = 0.78) and 0.2 ± 2.1 mm (p = 0.85), respectively.
Conclusions: Significant discrepancies between planned and actual femoral bone resection were demonstrated for flexion/extension angle, likely the result of cutting error. Our data highlights the importance of cut verification postresection to confirm planned resections are achieved, and suggests imageless navigation may be a source of feedback that would allow surgeons to intraoperatively adjust resections to achieve optimal implant alignment.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


